FOI 24/25- 0013
DOCUMENT 15
Research – Resources to assist with determining personal care
hours
We are seeking to see if there are any documents available that may assist with
determining personal care hours for
- A range of tasks
- range of disabilities
- different severity levels
Tasks include but not limited to:
Showering, dressing, toileting, eating, drinking, shaving etc.
E.g. People who are hoist transferred wil require more time to shower than
non-hoist transfer. People whom are fully dependent with a task wil require
Brief
more time than a person who can assist.
Please expand the scope to include disability health related supports
That is, time taken to change different catheter types, provide PEG feeds,
change wounds, perform suctioning etc.
Are there any state or commonwealth governments have these types of
guidelines? E.g. Insurance / compensation schemes, DVA, state disability
service providers prior to the NDIS???
Are there any professional guidelines that describe this?? (Likely to have some
in the health related tasks, but not sure for the personal care tasks???
Date
15/03/21
Requester(s)
Jane s22(1)(a)(ii)
- irre – ( Assistant Director - TAB)
Researcher
Jane s22(1)(a)(ii) - irrelev (R esearch Team Leader - TAB)
Cleared
N/A
Please note:
The research and literature reviews col ated by our TAB Research Team are not to be shared external to the Branch. These
are for internal TAB use only and are intended to assist our advisors with their reasonable and necessary decision-making.
Delegates have access to a wide variety of comprehensive guidance material. If Delegates require further information on
access or planning matters they are to call the TAPS line for advice.
The Research Team are unable to ensure that the information listed below provides an accurate & up-to-date snapshot of
these matters.
Page 141 of 425











FOI 24/25- 0013
Contents
Summary ......................................................................................................................................... 2
Spinal Cord Injury Guidelines .......................................................................................................... 2
3.1
Methods to develop guidance ................................................................................................ 3
How iCare NSW determines level of attendant care ...................................................................... 3
4.1
Requesting attendant care...................................................................................................... 4
Australian Community Industry Alliance ........................................................................................ 4
American Association on Intellectual and Developmental Disabilities Severity Codes .................. 4
Tools to assess individualised support needs ................................................................................. 5
7.1
Support Intensity Scale ........................................................................................................... 5
7.2
Classification and Assessment of Support Needs ................................................................... 6
Factors affecting support needs ..................................................................................................... 6
References ...................................................................................................................................... 6
Summary
There are no guidelines or documents in the support worker/attendant care or nursing (health
related supports) space that assist with determining the number of personal care hours required for
a range of tasks, disabilities or severity level.
Compensation schemes such as iCare NSW use the Care and Needs Scale (CANS) to determine
support needs, however, clinician experience as well as the assessment results are used to
determine the required hours for individual participants.
A systematic review has identified two assessment instruments, the Instrument for the Classification
and Assessment of Support Needs (I-CAN) and the Support Intensity Scale for assessing
individualized support planning and resource allocation. Both these assessment tools utilise rating
scales rather than specific ‘hours’ or ‘time’ required for each personal care or health related support.
TAB senior technical advisor Gavan s22(1)(a)(ii) - ir (nu rsing) was consulted about the existence of nursing
guidelines. To his knowledge, no guidelines exist.
Spinal Cord Injury Guidelines
The level of support tables in the spinal cord injury guidelines developed by iCare NSW provide an
estimate of need and care hours based on the level of the person’s injury. These are separated into:
1) Transfers and moving around
2) Self-care
3) Domestic life
Page 142 of 425

FOI 24/25- 0013
4) Participation in major areas of life
Total hours are provided across the sub-sections rather than individual task hours/time. For
example, there is substantial variation in the level of support a person with an injury at C7-C8 is
estimated to require. Including 14-21 hours of self-care/transfers and moving around, 7-21 for
domestic life and hours for participation in major areas of life are “dependent on the individual”.
Within the recommendations section it also states that:
Decisions about the need for assistance from support workers for a person with traumatic spinal
cord injury should consider knowledge and understanding of the:
• Person – goals, body function and structure, activities and participation, and the stage post
injury
• Person’s context – environmental, personal factors, attitudes, beliefs and social norms,
supports (informal and formal)
• Person’s progress – towards their goals, their outcomes, barriers and facilitators in the
person’s context.
On page 82 of the guideline this below statement is made:
There is no standard level of support. It’s not just about the level of the spinal cord injury nor who
lives with you and how they assist you. Each person has different life activities, goals, home and local
communities which can affect their need for support (page 82).
3.1
Methods to develop guidance
1) Systematic review of published literature
2) Survey of stakeholders
3) Analysis of the use of support workers by iCare Lifetime Care participants per year since
injury (total cost and average hourly rate)
4) Non peer reviewed information including international trends in spinal cord injury, support
worker industry information, frameworks and modelling for concepts of decision making
5) Working party of experts
6) Stakeholder feedback
7) Peer review of draft guidance
How iCare NSW determines level of attendant care
iCare uses the term ‘attendant care’ which refers to support worker services or community worker
services [1]. This covers
• personal care, such as showering or dressing
• domestic tasks, such as preparing meals and cleaning
• help to attend your injury-related treatment and rehabilitation activities or appointments
• support with engaging in family or community activities
• registered nursing assistance
• Gardening and general maintenance of your home.
Page 143 of 425


FOI 24/25- 0013
4.1
Requesting attendant care
A participant’s need for attendant care is assessed when entering in the Lifetime Care scheme and
periodical y as needed from that time [1]. A
care needs assessor, who is a health professional, such
as an occupational therapist, will identify the care needs. The care needs assessor meets with the
participant and family in their home to talk about the required care needs. They may also talk to the
case manager and any other service providers working with the participant to make sure that all
needs are understood.
The care needs assessor wil generate a report on the care needs of the participant and a request for
services to meet the care needs related to your injury.
The amount and type of attendant care iCare can pay for depends on:
• needs relating to the injury
• goals for what the participant wants to do
• personal and home circumstances
Australian Community Industry Alliance
The Australian Community Industry Al iance (formerly
Attendant Care Industry Association (ACIA) states that
support workers must [2]:
• Fol ow the plan as provided by the service provider
• Report to their supervisor of any changes or variations for advice
• Not change the plan
• Identify, and report to their supervisor, any gaps in their ability to deliver the required service
including difficulties in completing the tasks within the al ocated time
American Association on Intel ectual and
Developmental Disabilities Severity Codes
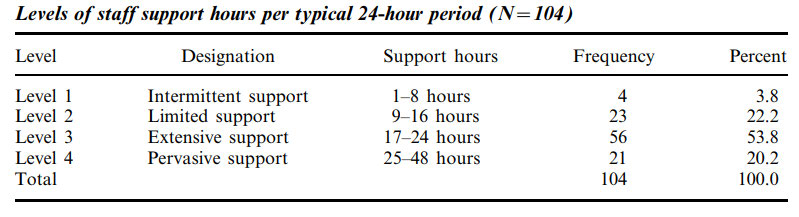
In the journal article by Riches [3] the American Association on Intellectual and Developmental
Disabilities (AAIDD) severity codes for intellectual disabilities were used to examine the support
needs of 104 participants in a community living environment across key domains. This was used to
determine resource al ocation and results can be found below.
The AAIDD severity codes are provided below [4].
Page 144 of 425

FOI 24/25- 0013
Intermittent support: Many people with intellectual disabilities do not require regular support or
assistance. Instead, they may only require additional supports during times of transition,
uncertainty, or stress. Usual y people requiring this level of support would be categorized under the
APA standards as mild intellectual disability.
Limited support: Some people with intellectual disabilities can learn to improve their adaptive
behaviour. With additional training, they can increase their conceptual skills, social skills, and
practical skills. However, they may still require additional support to navigate everyday situations.
People in this group would often be categorized by APA standards as moderate intellectual disability.
Extensive support: Other people with intellectual disability require support that is more intensive.
These individuals have some basic communication skills and can complete some self-care tasks.
However, they will usually require daily support. This level of support is usually associated with
severe intellectual disability by APA criteria.
Pervasive support: Pervasive support describes the most intense level of support. Daily
interventions are necessary to help the individual function. Supervision is necessary to ensure their
health and safety. This lifelong support applies to nearly every aspect of the individual's routine. This
classification is associated with those who have profound intellectual disability.
Tools to assess individualised support needs
A systematic review by Verdugo, Aguayo [5] aimed to analyse the rigor and usefulness of the
available standardized tools for assessing support needs and found that only the Support Intensity
Scale (SIS) and the I-CAN have been used for individualized support planning and resource allocation.
7.1
Support Intensity Scale
The SIS provides ratings across three dimensions of support needs –
frequency, daily support time
and type of support [6, 7].
1) Frequency rating options are:
a. 4= hourly or more frequently
b. 3=at least once a day but not once an hour
c. 2=at least once a week, but not once a day;
d. 1=at least once a month, but not once a week
e. 0=none or less than monthly
2) Daily support time rating options are:
a. 4=4 hours or more
b. 3=2 hours to less than 4 hours
c. 2=30 minutes to less than 2 hours
d. 1=less than 30 minutes
e. 0=none
3) Type of support rating options are:
a. 4=full physical assistance
b. 3=partial physical assistance
c. 2=verbal/gestural prompting
Page 145 of 425


FOI 24/25- 0013
d. 1=monitoring
e. 0=none.
7.2
Classification and Assessment of Support Needs
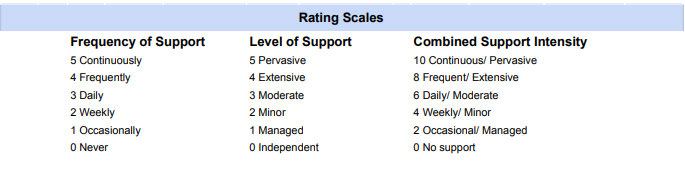
Questions in the I-CAN are rated using two 0-5 point scales [5, 7]. The Frequency of Support scale
asks how often support is needed. The Level of Support scale asks how much support is needed.
These two scales are added to give a 0-10 Combined Support Intensity scale. Figure 1 shows the
rating scale for the I-CAN
Figure 1: I-CAN rating scale.
Factors affecting support needs
The systematic review by Verdugo, Aguayo [5] provides various factors that affect level of support
needs including:
• Age
• Level of intellectual disability
• Adaptive behaviour skills
• Number and type of associated disabilities
• Medical and behavioural needs
References
1.
Insurance & Care NSW. Attendant care for people with a severe injury 2020 [Available from:
https://www.icare.nsw.gov.au/injured-or-ill-people/motor-accident-injuries/attendant-
care/working-with-an-attendant-care-provider#gref.
2.
Australian Community Industry Alliance. ACIA 030 – Supporting Persons with Dysphagia at
Mealtimes in the Community 2020 [Available from: https://acia.net.au/wp-
content/uploads/2020/10/ACIA-030-Guideline-for-Supporting-Persons-with-Dysphagia-at-
mealtimes-in-the-Community-002.pdf.
3.
Riches VC. Classification of support needs in a residential setting. Journal of Intellectual &
Developmental Disability [Internet]. 2003 2003/12/01; 28(4):[323-41 pp.]. Available from:
https://doi.org/10.1080/1366825031000150982.
4.
Shogren KA, Turnbull HR. Public policy and outcomes for persons with intellectual disability:
extending and expanding the public policy framework of AAIDD's 11th Edition of Intel ectual
Page 146 of 425
FOI 24/25- 0013
Disability: Definition, Classification, and Systems of Support. Intellect Dev Disabil [Internet]. 2010
Oct; 48(5):[375-86 pp.].
5.
Verdugo MA, Aguayo V, Arias VB, García-Domínguez L. A Systematic Review of the
Assessment of Support Needs in People with Intel ectual and Developmental Disabilities.
International journal of environmental research and public health [Internet]. 2020; 17(24):[9494 p.].
Available from: https://pubmed.ncbi.nlm.nih.gov/33352974.
6.
American Association on Intellectual and Developmental Disabilities. Supports Intensity
Scale Scoring Clarifications & Frequently Asked Questions 2008 [Available from:
https://www.aaidd.org/docs/default-source/sis-
docs/sisfrequencyandscoringclarifications.pdf?sfvrsn=9258607d 2.
7.
Arnold SRC, Riches VC, Stancliffe RJ. I-CAN: The Classification and Prediction of Support
Needs. Journal of Applied Research in Intellectual Disabilities [Internet]. 2014 2014/03/01; 27(2):[97-
111 pp.]. Available from: https://doi.org/10.1111/jar.12055.
Page 147 of 425