 DOCUMENT 1
DOCUMENT 1
FOI 23/24-1268
Research Request – Oedema and Lymphoedema Management
Brief
Oedema and Lymphoedema. Best Practice Management.
Date
January 10, 2020
Requester
Wendy
(
s22(1)(a)(ii) Dire ctor – TAB)
Researcher
Craig s22(1)(a)(ii) - i (Tac tical Research Advisor – TAB/AAT)
Contents
SUMMARY ............................................................................................................................................... 2
DIFFERENCE BETWEEN OEDEMA AND LYMPHOEDEMA ......................................................................... 3
OEDEMA .................................................................................................................................................. 4
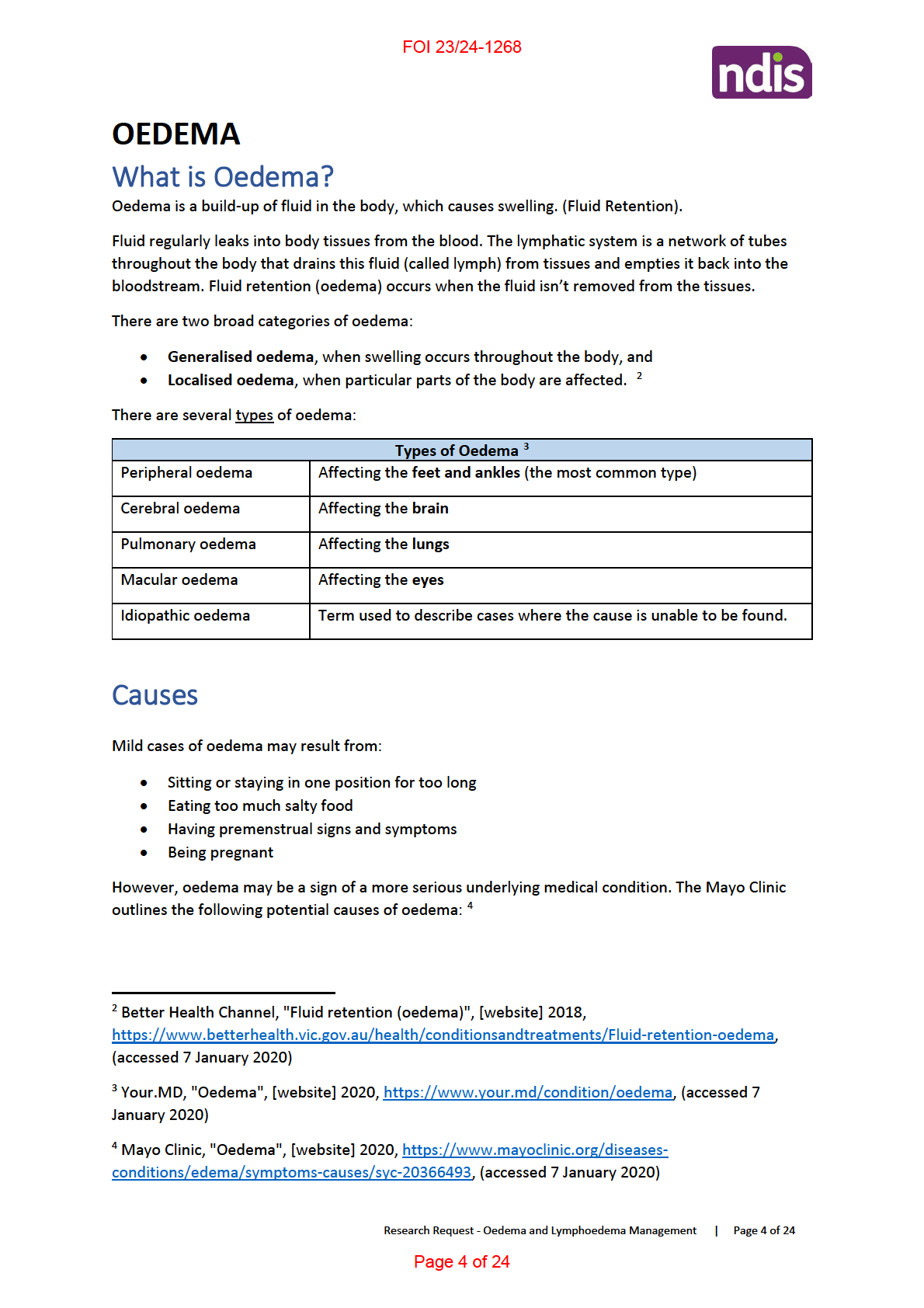
What is Oedema? ................................................................................................................................ 4
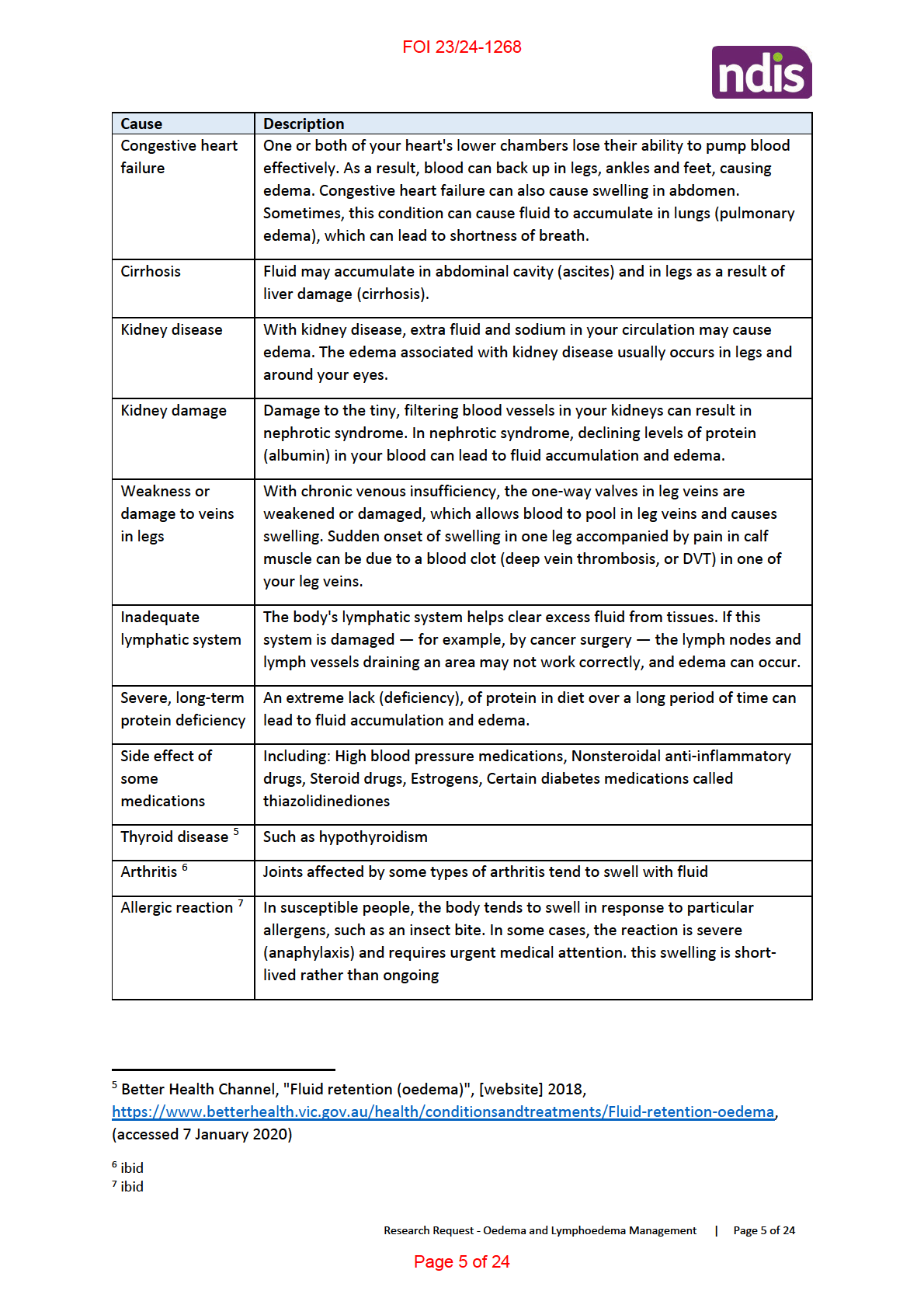
Causes ................................................................................................................................................. 4
Management ....................................................................................................................................... 6
Functional Capacity ............................................................................................................................. 7
Permanency & Early Intervention ....................................................................................................... 7
LYMPHOEDEMA ...................................................................................................................................... 7
What is Lymphoedema? ..................................................................................................................... 7
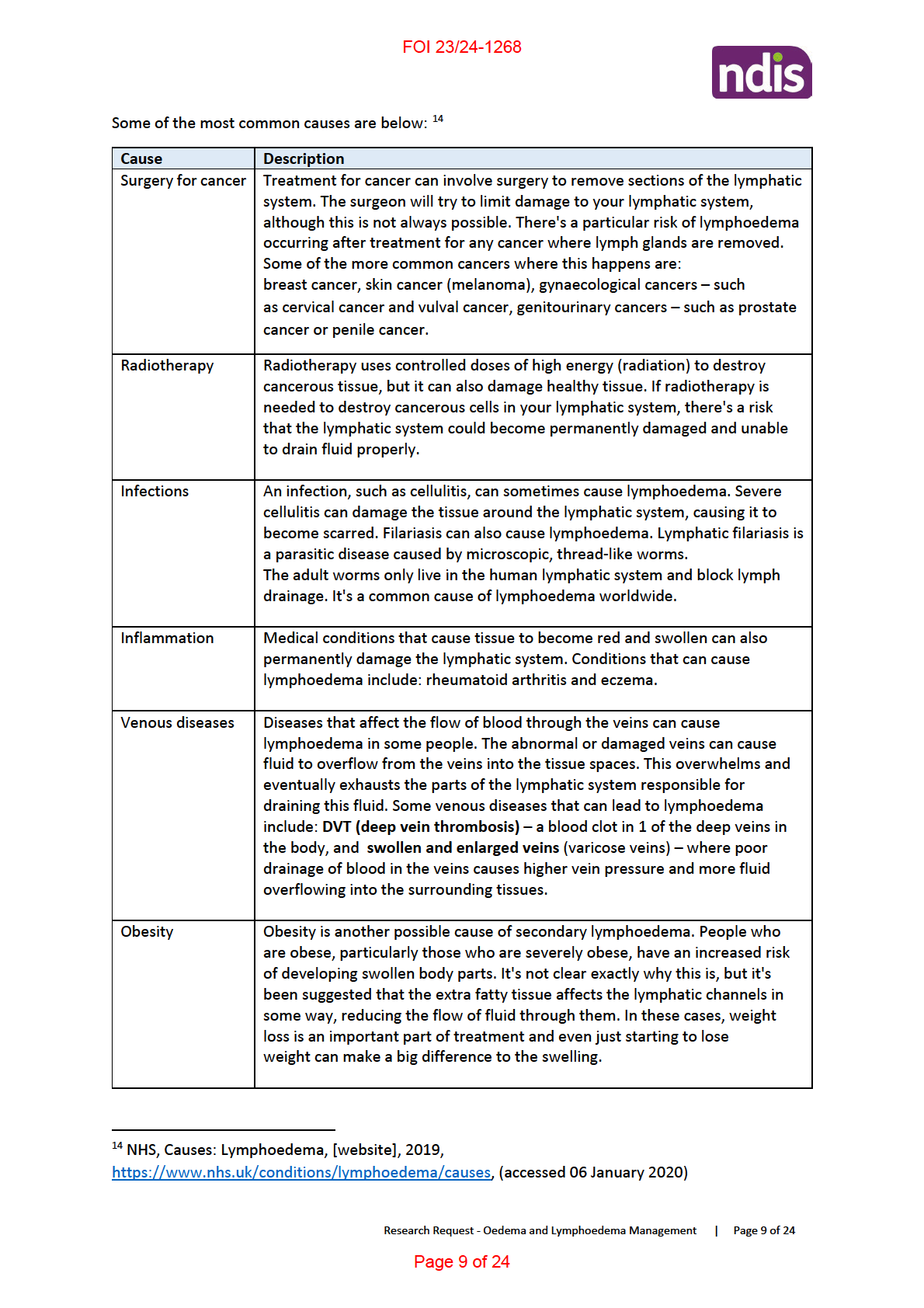
Causes ................................................................................................................................................. 8
Management ..................................................................................................................................... 10
Skin Care and Cellulitis/erysipelas ................................................................................................ 11
Lymphatic Massage ....................................................................................................................... 12
Intermittent Pneumatic Compression (IPC) .................................................................................. 12
Multi-layer Inelastic Lymphoedema Bandaging (MLLB) ............................................................... 12
Compression Garments (Long Term Management) ..................................................................... 13
Exercise/movement and Elevation ............................................................................................... 14
Psychosocial Support .................................................................................................................... 14
Palliative Care ............................................................................................................................... 15
Surgery .......................................................................................................................................... 15
Other Treatments ........................................................................................................................ 16
Other recent management investigations .................................................................................... 17
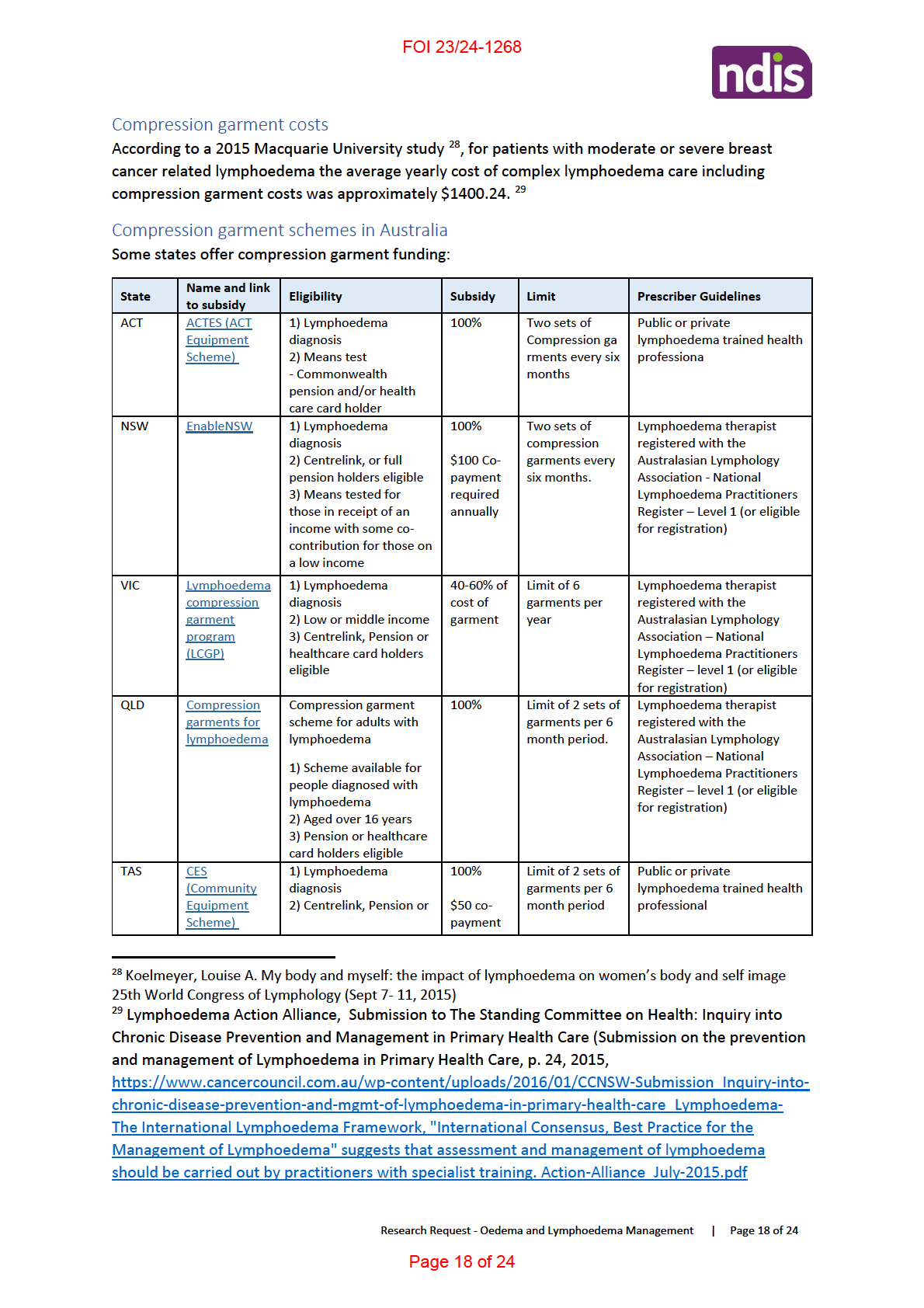
Costs of Lymphoedema Management .............................................................................................. 17
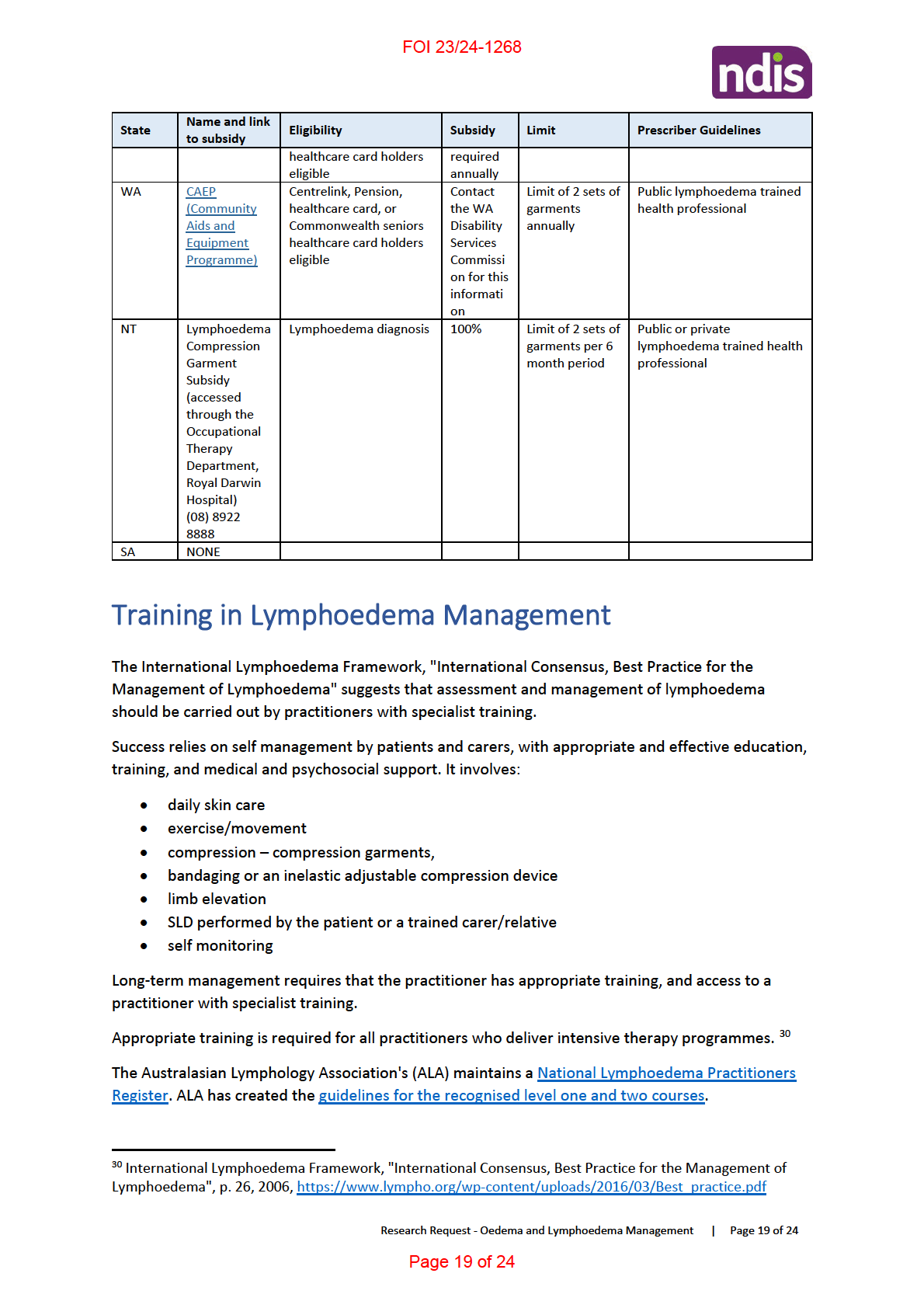
Training in Lymphoedema Management .......................................................................................... 19
Functional Capacity ........................................................................................................................... 20
Research Request - Oedema and Lymphoedema Management | Page 1 of 24
Page 1 of 24

FOI 23/24-1268
Mobility and functional assessment ............................................................................................. 20
Psychological Functioning ............................................................................................................. 20
Social Functioning ......................................................................................................................... 21
Other functional impacts on the patient ...................................................................................... 21
Permanency & Early Intervention ..................................................................................................... 22
Reference List ........................................................................................................................................ 23
Please note:
The research and literature reviews col ated by our TAB Research Team are not to be shared external to the Branch. These
are for internal TAB use only and are intended to assist our advisors with their reasonable and necessary decision making.
Delegates have access to a wide variety of comprehensive guidance material. If Delegates require further information on
access or planning matters they are to call the TAPS line for advice.
The Research Team are unable to ensure that the information listed below provides an accurate & up-to-date snapshot of
these matters.
SUMMARY
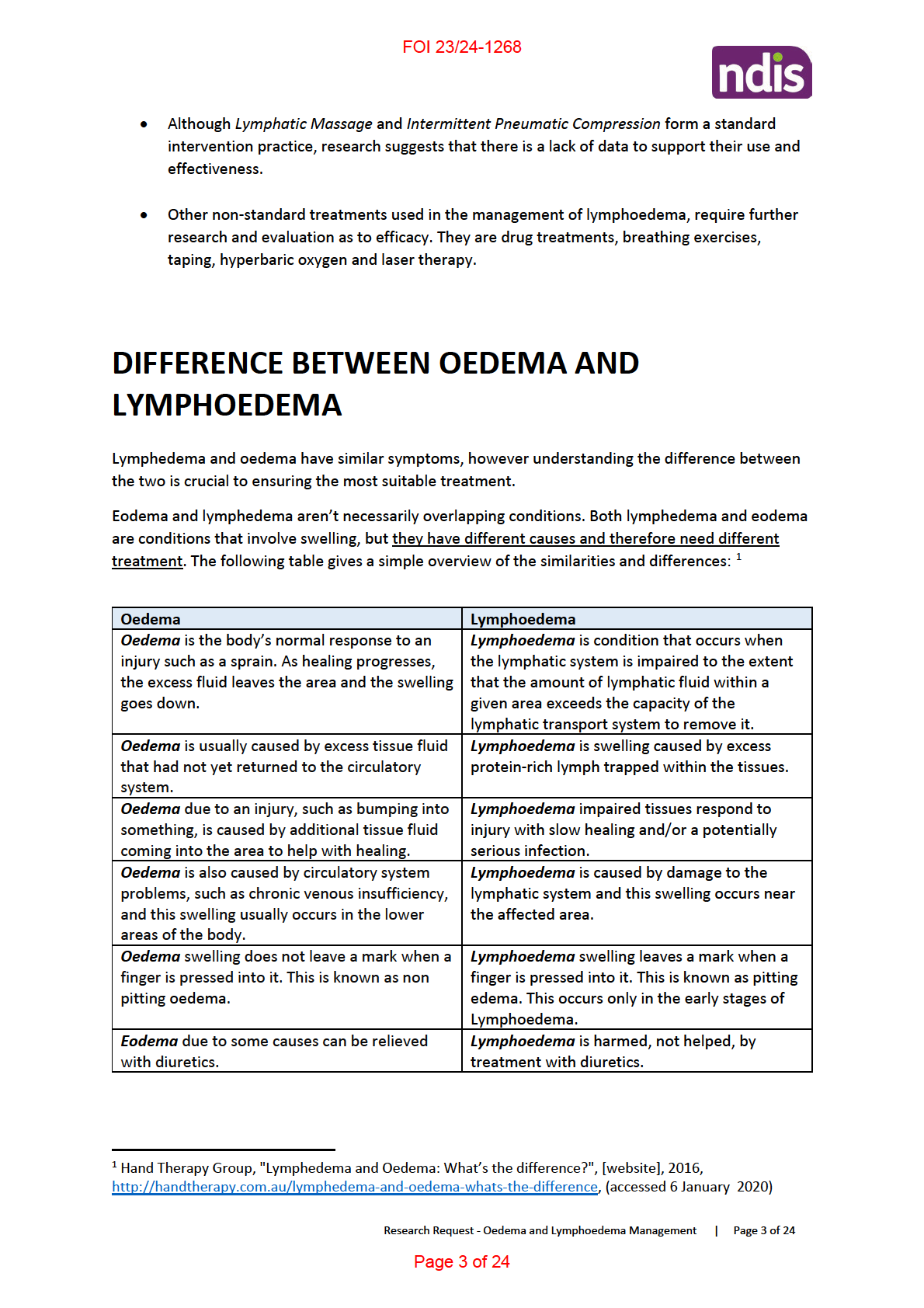
• Lymphoedema and oedema (American spelling: Lymphedema and edema) have similar
symptoms, however understanding the difference between the two is crucial to ensuring the
most suitable treatment.
• Research indicates that oemeda appears not to be a permanent condition and can be
managed successful y with appropriate treatment. However this depends on what might be
causing the condition.
• Research indicates that lymphoedema appears to be a permanent condition and that
management of the condition focuses on reducing the swelling and control ing the pain.
• Best practice management of lymphoedema has a holistic, multidisciplinary approach, and
Australian best practice management relies largely on the "International Lymphoedema
Framework: Best practice in the Management of Lymphoedema".
• The aims of lymphoedema management are to prevent progression of the condition, to
reduce odema and then maintain the improvement.
• Whilst there are several standard management interventions for lymphoedema,
compression garments are recognised as a long term management intervention.
• High costs to the patient are associated with compression garments, however most
Australian states offer a subsidy scheme.
Research Request - Oedema and Lymphoedema Management | Page 2 of 24
Page 2 of 24

FOI 23/24-1268
Functional Capacity
Depending on the extent of the condition (including category and type), functional capacity for those
suffering from oedema wil be comparable to that of those suffering from Lymphoedema. See
“Lymphoedema: Functional Capacity” below.
Permanency & Early Intervention
Research indicates that oedema may not be a permanent condition and can be managed
successful y with appropriate treatment. However this depends on what might be causing the
condition:
“If there is an underlying cause for the dependent edema, then treating the condition may resolve
the edema. Sometimes, these conditions are not curable such as in the case of heart failure, so
people may need to manage the edema to limit its symptoms and reduce the risk of complications”.
10
LYMPHOEDEMA
What is Lymphoedema?
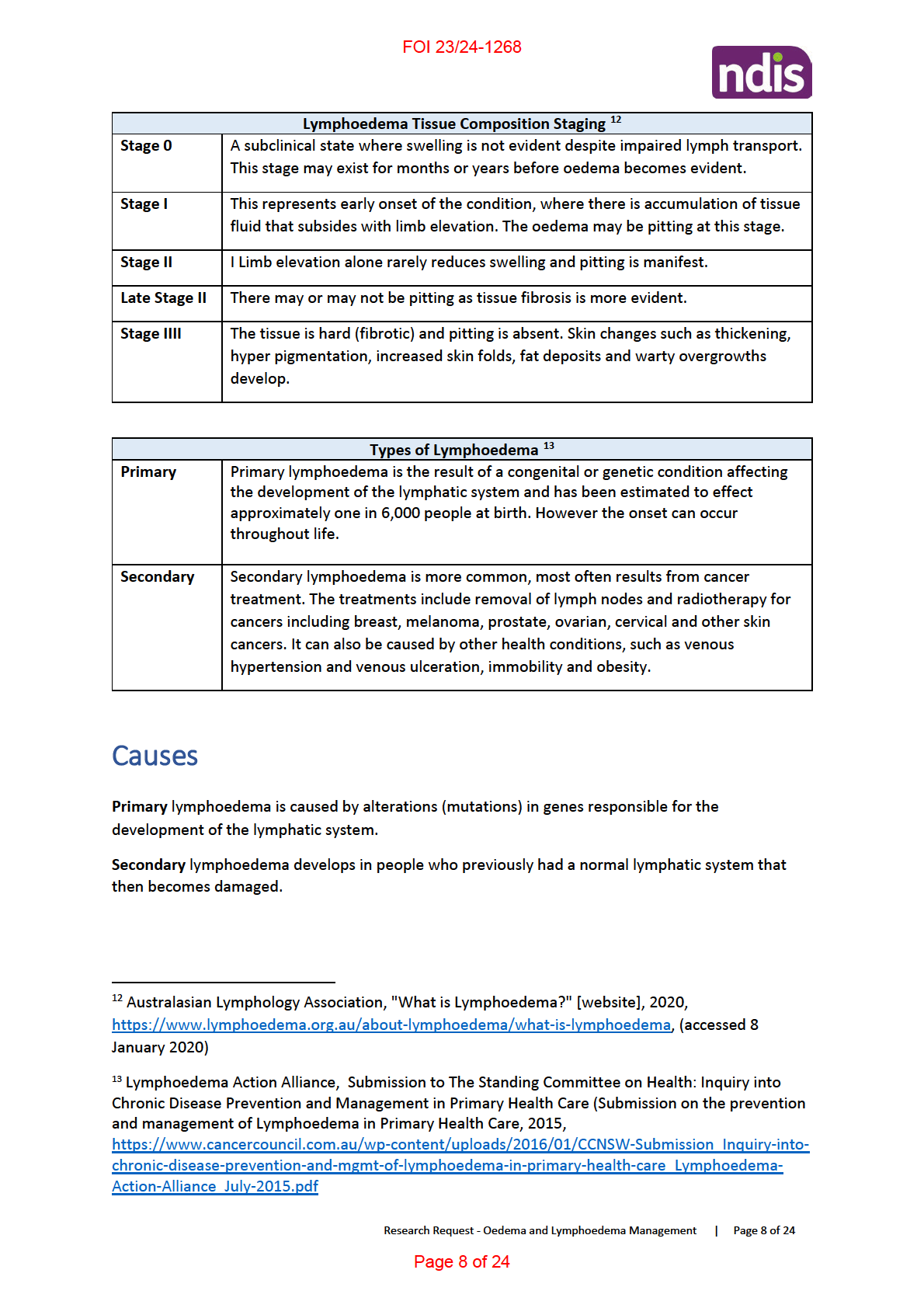
Lymphoedema is a chronic swelling of one or more limbs or body regions, such as the arms, legs and
neck, breast or genitals. Lymphoedema occurs when there is an imbalance in the transportation
and/or production of fluid in the interstitial tissues, resulting in the accumulation of extracellular
fluid. It may be a congenital malformation of the lymphatic system (primary lymphoedema) and/or
due to damage, trauma or interference with the lymphatic vessels or nodes, for example after
cancer treatment (secondary lymphoedema). While lymphoedema starts as a fluid focused
condition, for some, it can progress to accumulation of adipose and/or fibrotic tissue in affected
regions. This change in tissue composition is also known as staging, with lymphoedema currently
divided into four stages depending on the progression of the tissue change. 11
10 Medical News Today, "What is dependent edema?", [website], 2020,
https://www.medicalnewstoday.com/articles/320986.php, (accessed 10 January 2020)
11 NSW Government, Agency for Clinical Innovation, "Lymphoedema: A guide for clinical services",
2018, https://www.aci.health.nsw.gov.au/ data/assets/pdf file/0008/477998/lymphoedema-
guide.pdf
Research Request - Oedema and Lymphoedema Management | Page 7 of 24
Page 7 of 24

FOI 23/24-1268
Phase I – Intensive treatment consists of daily:
• Skin care to optimise the condition of the skin, reverse skin changes and treat infections.
• Manual Lymphatic Drainage (MLD) to enhance lymph flow. This precedes bandaging and
directs lymph fluid to functioning lymphatic territories and helps to establish collateral
drainage pathways.
• Application of multi-layer compression bandaging.
• Exercises to increase lymphatic and venous flow.
• Psychosocial support.
• A compression garment is prescribed, following a successful reduction. This is essential to
preserve the reduction achieved by treatment and to help prevent progression of the
lymphoedema.
• Education is incorporated to ensure that the client understands their condition and al parts
of the intensive treatment as well as the importance of phase II.
Phase II - Home maintenance programme
• Patients are educated by their therapist in the need for self-management to maintain the
results achieved in Phase I. Without the active involvement of the client, the successful
outcome of treatment may not be sustained.
• The routine adopted may vary from person to person but wil usual y include daily skin care
and prevention of infection, regular self massage, exercises and the wearing of the
prescribed compression garment(s).
• Patients encouraged to practice self monitoring and adopt a healthy lifestyle that includes
attention to diet, fitness and weight management.
• At times this treatment may be offered in a modified form to accommodate particular
individual needs.
Skin Care and Cellulitis/erysipelas
Swelling may produce deep skin folds where fungal and bacterial infections can develop. Chronic
inflammation causes deposition of fibrin and col agen, contributing to skin thickening and firm tissue
consistency. Reduced tissue compliance may further compromise lymph flow and increase the
tendency to infection. Maintenance of skin integrity and careful management of skin problems in
patients with lymphoedema are important to minimise the risk of infection. The general principles of
skin care aim to preserve skin barrier function through washing and the use of emol ients. Ordinary
soaps, which usual y contain detergents and no glycerin, should be avoided because they tend to dry
the skin. Natural or pH neutral soap can be used. The perfumes and preservatives in scented
products may be irritant or al ergenic. In high concentrations, mineral and petrolatum based
products may exacerbate dry skin conditions by occluding skin pores and preventing natural oils
from surfacing. 15
15 International Lymphoedema Framework, "International Consensus, Best Practice for the
Management of Lymphoedema", p 24, 2006, https://www.lympho.org/wp-
content/uploads/2016/03/Best practice.pdf
Research Request - Oedema and Lymphoedema Management | Page 11 of 24
Page 11 of 24

FOI 23/24-1268
Lymphatic Massage
Manual lymphatic drainage (MLD) is a gentle massage technique that is recognised as a key
component of decongestive therapy. MLD aims to encourage fluid away from congested areas by
increasing activity of normal lymphatics and bypassing ineffective or obliterated lymph vessels.
Although there is a wealth of clinical opinion advocating the benefits of MLD, there are little
research data to conclusively support its use. The most appropriate techniques, optimal frequency
and indications for MLD, as wel as the benefits of treatment, all remain to be clarified. MLD remains
a specialist skill that needs regular practice in order to maintain competence. Deep, heavy-handed
massage should be avoided because it may damage tissues and exacerbate oedema by increasing
capillary filtration. 16
Intermittent Pneumatic Compression (IPC)
Although there is considerable international debate over its effectiveness in lymphoedema,
intermittent pneumatic compression (IPC) is widely used. It may form part of an intensive therapy
regimen or long-term management in selected patients, and may be use.
IPC consists of an electrical air compression pump attached to an inflatable plastic garment that is
placed over the affected limb. The garment is inflated and deflated cyclically for a set period, usually
about 30-120 minutes. The pressure produced by the garment can be varied. Garments may be
single chambered, or contain multiple chambers (usually three, five or 10) that are inflated
sequential y to provide a peristaltic massaging effect along the length of the limb towards its root.
The question of whether single or multichambered devices are more effective remains open.
However, multichambered devices are used most frequently and randomised controlled trials have
shown them to produce a faster effect. IPC is thought to reduce oedema by decreasing capil ary
filtration, and therefore lymph formation, rather than by accelerating lymph return. IPC is
particularly effective in nonobstructive oedemas, eg those due to immobility, venous incompetence,
lymphovenous stasis or hypoproteinaemia. In obstructive lymphoedema, ie lymphoedema resulting
from lymphatic vessel/node damage or lymph node resection, SLD or MLD is recommended before
IPC to stimulate lymphatic flow. It is important that compression therapy with garments or
bandaging is continued after IPC to prevent rapid rebound swelling. 17
Multi-layer Inelastic Lymphoedema Bandaging (MLLB)
Multi-layer lymphoedema bandaging (MLLB) is a key element of intensive therapy regimens. For
some patients it may also form part of their transition, long-term or palliative management. MLLB
uses inelastic bandages that have low extensibility and that produce high working pressures and
lower resting pressures, ie they create peak pressures that produce a massaging effect and stimulate
lymph flow. In certain situations, elastic bandages may be used instead. Elastic bandages produce
sustained compression with smal er variations during movement.
As well as reducing oedema, MLLB:
• restores shape to the limb/affected area
• reduces skin changes such as hyperkeratosis and papil omatosis
• supports overstretched inelastic skin
• eliminates lymphorrhoea
16 Ibid, p 29
17 Ibid, p 31
Research Request - Oedema and Lymphoedema Management | Page 12 of 24
Page 12 of 24

FOI 23/24-1268
• softens subcutaneous tissues. MLLB is indicated when skin changes are marked or limb
distortion and skin folds preclude compression garments.
Contraindications to MLLB include severe peripheral arterial occlusive disease.
MLLB regimens can be adapted to individual patient's needs by varying the:
• pressure produced by the bandages
• frequency of bandage change
• bandage bulk
• type of bandage, eg using elastic bandages instead of inelastic bandages.
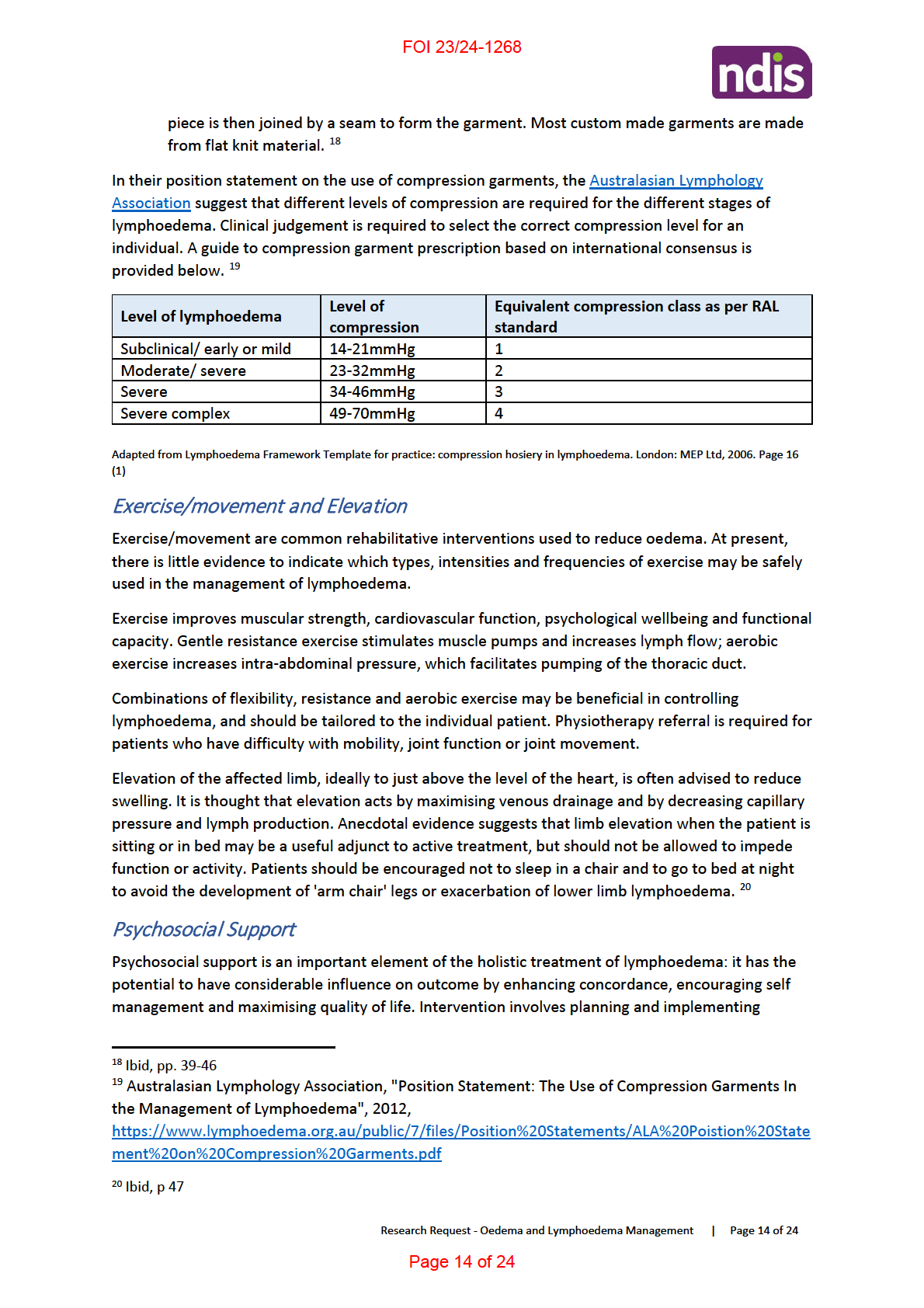
Compression Garments (Long Term Management)
The main use of compression garments is in the long-term management of lymphoedema, usual y
following a period of intensive therapy. Compression garments are also used for prophylaxis or as
part of initial treatment. They may provide the only form of compression used, or form part of a
regimen that includes other types of compression. Some patients wear garments during waking
hours only, for exercise only, or up to 24 hours per day. A wide variety of factors must be taken into
account when determining whether a patient is suitable for compression garments.
Criteria indicating patient suitability for compression garments:
• Good dexterity
• Intact, resilient skin
• No or minimal shape distortion
• Absent or minimal pitting oedema
• Swelling that can be contained by compression garments
• Concordant and motivated
• Ability to tolerate and manage hosiery (+/- carer support)
• Ability to monitor skin condition and engage in prevention strategies
• Symptom-based management/pal iative needs
Contraindications to compression garments:
• Arterial insufficiency - ABPI <0.5 in the lower limb
• Acute cardiac failure
• Extreme shape distortion
• Very deep skin folds
• Lymphorrhoea, or other weeping skin condition
• Extensive ulceration
• Severe peripheral neuropathy
Compression garments can be categorised according to method of fabric manufacture:
•
Circular knit garments – the material is continuously knitted on a cylinder and has no seam,
and is used mainly to make ready to wear garments. Garments are shaped by varying stitch
height and yarn tension. Circular knit garments may be thinner and more cosmetical y
acceptable than flat knit garments.
•
Flat knit garments – the material is firmer and thicker than that of circular knit garments.
Garments are knitted as a flat piece that is shaped by adding or removing needles. The flat
Research Request - Oedema and Lymphoedema Management | Page 13 of 24
Page 13 of 24

FOI 23/24-1268
psychosocial care strategies that help patients and their family/carers to take a positive role in the
management of their lymphoedema and to achieve as good a quality of life as possible. If
psychosocial problems are not resolved within three months, the patient should be referred for
specialist intervention. 21
Palliative Care
The needs of patients with lymphoedema who are otherwise ill with advanced disease and who
require pal iative care can be complex. This document can provide only an indication of supportive
measures and treatments that may be helpful. Lymphoedema can produce distressing and
debilitating symptoms that affect lifestyle and function. Patients with advanced disease may not be
able to tolerate a full programme of assessment and treatment, but require a pal iative approach in
which assessment techniques are modified and individual treatments are selected to ease specific
symptoms. 22
Surgery
Surgical treatment of lymphoedema can be divided into three main categories:
1. Surgical reduction
2. Procedures that bypass lymphatic obstructions
3. Liposuction.
Patients for surgery need to be selected carefully and counselled to ensure realistic expectations of
likely outcome. Maintenance of any improvement gained requires long-term postsurgical
compression therapy.
Surgical reduction (sometimes also known as debulking surgery) aims to remove excess
subcutaneous tissue and skin, and may be useful in the symptomatic treatment of severe
lymphoedema. However, the postsurgical morbidity of reduction operations may be considerable. In
some cases, surgical reduction may be considered for lymphoedema of the eyelid or genitalia.
Bypass operations aim to restore lymphatic function through lymphovenous anastomoses and
lymphatic or venous vessel grafting, or lymph node transplantation. Anastomosis of lymph vessels to
the venous system may be attempted in patients with proximal lymphatic obstruction and patent
distal lymphatics, and produces better results at earlier stages of lymphostatic disease. Lymphatic
grafting and lymph node transplantation require microsurgical techniques, and show promising
results in carefully selected patients.
Liposuction in patients with chronic lymphoedema, adipocyte proliferation (which may be related to
an inflammatory process) may mean that conservative treatment or microsurgery do not completely
resolve limb enlargement. Liposuction has been performed on patients with long-standing breast
cancer related lymphoedema. It removes excess fat tissue and is considered only if the limb has not
responded to standard conservative therapy. Liposuction does not correct inadequate lymph
drainage and is not indicated when pitting is present. Where concordance with compression
garments after treatment is high, results have been maintained. Liposuction has also been used for
primary and secondary leg lymphoedema with promising results. 23
21 Ibid, p 48
22 Ibid, p 49
23 Ibid, p 50
Research Request - Oedema and Lymphoedema Management | Page 15 of 24
Page 15 of 24

FOI 23/24-1268
Other Treatments 24
A variety of other treatment modalities may be used to treat lymphoedema; many require further
evaluation:
Drug Treatment
Two main groups of drug have been used in the treatment of lymphoedema: benzopyrones and
diuretics.
Benzopyrones are based on a variety of natural y occurring substances. Examples include flavonoids,
oxerutins, escins, coumarin, and ruscogen combined with hesperidin. There is little evidence to
support the use of these drugs in lymphoedema. There is some data, however, that flavonoids may
stabilise swel ing by reducing microvascular filtration.
Diuretics encourage the excretion of salt and water, and by reducing blood volume might be
expected to reduce capil ary filtration and lymph formation. There is no evidence that diuretics
encourage lymph drainage. A diuretic is likely to be prescribed on a pragmatic basis for anyone with
oedema almost irrespective of cause.
Breathing Exercises
Breathing exercises are recommended by some clinicians as a preliminary manoeuvre that may help
to clear the central lymphatics prior to interventions that promote lymph drainage from the
peripheries. However, other clinicians question the physiological basis of breathing exercises as
there are no experimental data in humans to confirm that variations in intrathoracic pressure due to
breathing assist central lymphatic drainage into the venous system.
Lymphoedema taping
Lymphoedema taping is an emerging form of treatment for lymphoedema. It involves the
application of narrow strips of elastic tape to the affected area, and can be used in combination with
compression garments or bandaging. It is thought to improve muscle function and lymph flow and
may have a role to play in the treatment of midline and peripheral swelling. However, evidence is
lacking of its efficacy in lymphoedema.
Hyperbaric oxygen
Hyperbaric oxygen therapy is known to promote healing in bone that has become ischaemic
fol owing radiotherapy. In patients with upper limb lymphoedema fol owing radiotherapy, two smal
studies have indicated that hyperbaric oxygen may improve lymph flow and reduce limb volume in
the short-term. Further research is required to establish whether benefits can be demonstrated in
randomised trials and in the long-term.
Laser Therapy
Low level laser therapy has shown potential for the treatment of lymphoedema, particularly of the
upper limb, where it has reduced limb volume and tissue hardness101. Further research is required
to establish the benefits of treatment and the optimal regimen.
24 Ibid, p 50
Research Request - Oedema and Lymphoedema Management | Page 16 of 24
Page 16 of 24

FOI 23/24-1268
Other recent management investigations
Hydrotherapy
A recent 2017 clinical review paper suggests that there is a role for Contrast Hydrotherapy in the
management of lymphoedema. The paper suggests that "The majority of conventional treatments
for the management of lymphoedema are conservative, with their primary aim being a reduction in
the volume of the affected limb, to restore function and quality of life"
The paper outlines that whilst the concept is theoretical based, hydrotherapy may prove to be an
effective treatment for lymphoedema, and that clinical investigation with pilot trials is warranted. 25
Another case study research article suggests that hydrotherapy effectiveness results from the ability
of water’s hydrostatic pressure to remove fluid and of self-massage and exercises to promote
protein removal and clearance through use of healthy lymphotomes. The activities that patients
follow as they treat themselves include muscular exercise, which contrasts with conventional
treatments that use passive techniques. 26
Costs of Lymphoedema Management
In 2012, the International Lymphoedema Framework Australia conducted the largest lymphoedema
stakeholder survey ever done internationally. It identified the following key issues to improve the
treatment and management of lymphoedema in Australia: 27
• A need for education about lymphoedema, especially for medical professionals, allied health
professionals, and the community.
• The lack of services to meet patient’s needs, including the availability of services, time taken
to access services, as well as rural and public services. This included the lack of links between
the medical profession and therapists, (referral process and maintenance of patients care),
inadequate pathways to service, and limited resources that prevent patients from getting
timely and appropriate access to services.
• High cost of treatment including lack of government funding of treatments and general cost
of accessing appropriate treatment.
• High cost of compression garments.
25 P. Baker, "Is there a role for contrast Hydrotherapy", Journal of Lymphoedema, Vol 6, No 2, 2011,
https://www.woundsinternational.com/uploads/resources/content 11212.pdf
26 D. Tidhar et al., "Aqua Lymphatic Therapy in Managing Lower Extremity Lymphedema", J Support
Oncol, Vol 5, pp. 179-183, 2007, http://www.aqua-lymphatic-
therapy.com/files/Aqua Lymphatic Therapy in Managing Lower Extremity Lymphedema.pdf
27 Lymphoedema Action Alliance, Submission to The Standing Committee on Health: Inquiry into
Chronic Disease Prevention and Management in Primary Health Care (Submission on the prevention
and management of Lymphoedema in Primary Health Care, 2015, p8,
https://www.cancercouncil.com.au/wp-content/uploads/2016/01/CCNSW-Submission Inquiry-into-
chronic-disease-prevention-and-mgmt-of-lymphoedema-in-primary-health-care Lymphoedema-
Action-Alliance July-2015.pdf
Research Request - Oedema and Lymphoedema Management | Page 17 of 24
Page 17 of 24

FOI 23/24-1268
The following courses are open to Medical Practitioners, Physiotherapists, Occupational Therapists,
Registered Nurses, and Remedial Massage Therapists, and are provided by various ALA registered
training providers:
• Level 1 courses provide the practitioner with the basic skills/knowledge to assess and treat
uncomplicated lymphoedemas.
• Level 2 courses provide the practitioner with the training to assess and treat all forms of
lymphoedema including complex presentations. 31
Functional Capacity
Mobility and functional assessment
The International Consensus on best practice management of lymphoedema suggests that the
assessment of a patient's mobility and functional status wil contribute to the formulation of a
management plan, and determine whether referral for further assessment is necessary.
Functional assessment of lymphoedema affecting the head, neck, trunk or genitalia should be
undertaken by a lymphoedema specialist. Functional assessment of limbs will include:
ARM:
• range of joint movement
• ability to use fastenings, eg buttons, bra fastenings
• ability to put on or remove underwear/compression garments or bandaging
• hand grip and pincer movement
• effect of lymphoedema on activities of daily living
• use of any aids
LEG:
• range of joint movement
• ability to get up from sitting or lying
• ability to walk; gait analysis
• ability to lift individual legs
• posture when sitting and standing
• ability to put on and take off footwear/compression garments or bandaging
• suitability of footwear
• effect of lymphoedema on activities of daily living
• use of any aids
Psychological Functioning
31 Australasian Lymphology Association, "Training in Lymphoedema Management", [website], 2020,
https://www.lymphoedema.org.au/the-register/lymphoedema-training-courses, (accessed 6
January 2020)
Research Request - Oedema and Lymphoedema Management | Page 20 of 24
Page 20 of 24

FOI 23/24-1268
Psychological assessment will include asking the patient how their swelling makes them feel about
themselves alongside assessment for:
• depression – eg low mood, loss of interest, low energy, changes in weight, appetite or sleep
patterns, poor concentration, feelings of guilt or worthlessness, suicidal thoughts
• anxiety – eg apprehension, panic attacks, irritability, poor sleeping, situation avoidance, poor
concentration
• cognitive impairment – may contribute to lack of motivation and inability to be independent
• lack of motivation
• ability to cope
• understanding of disease and concordance with treatment. 32
Social Functioning
Social factors assessed include:
• accommodation – accessibility, general living standards, heating/cooling
• support – involvement of carers, effect of lymphoedema on personal relationships, social
isolation
• employment – ability to work, effect of work on lymphoedema
• education – ability to attend educational establishment and study
• financial status – benefit entitlement, medical insurance
• recreational activities, exercise, sport. 33
Other functional impacts on the patient
Physical
• Lymphoedema can cause pain, and decreased limb movement and mobility.
• It can cause problems with dressing and other activities of daily living.
• Oversized clothing and footwear, needed to accommodate a swol en limb or body part,
present fall risks and significant difficulties in mobilisation.
• Lymphoedema may also cause chronic skin changes, reducing the skin’s ability to act as a
barrier to infections (cellulitis) and increasing the challenges of treating wounds.
• Left untreated, patients with lymphoedema are twice as likely to develop cellulitis requiring
hospitalisation and intravenous antibiotic therapy. 34
• Impaired mobility - edematous limb shifts center of gravity which when combined with
difficulty finding footwear result in limits range of motion, impaired footwear, increased fall
risk. 35
32 ibid
33 ibid
34 NSW Government, Agency for Clinical Innovation, "Lymphoedema:
A guide for clinical services", 2018, p 4,
https://www.aci.health.nsw.gov.au/ data/assets/pdf file/0008/477998/lymphoedema-guide.pdf
35 S. Ehmann and K. Bock, "Functionality to measure outcomes for safety, effectiveness and cost
implications" (New Frontiers in Wound Management New Frontiers in Wound AND Edema
Management, EWMA), 2018, https://ewma.org
Research Request - Oedema and Lymphoedema Management | Page 21 of 24
Page 21 of 24

FOI 23/24-1268
Psychological
• Resulting in negative body image, emotional disturbances, anxiety and depression, as wel as
social isolation.
• In a national survey, supported by Breast Cancer Network Australia, a diagnosis of
lymphoedema impacted work, family life, self-image and feelings.
• The greater the severity of lymphoedema, the higher the impact on the individual.
• Adolescents and young people with lymphoedema also experience issues with social
inclusion and participation with peers, poor self-image and emotional disturbances.
• Further chal enges identified for the families of children with lymphoedema include: altered
relationships between parents and children with lymphoedema (moving between being a
parent, an advocate, and a proxy health professional), as wel as altered relationships
between siblings (jealousy and time availability, also increased expectations of responsibility
and maturity, particularly for older siblings without lymphoedema). 36
Economic
• People living with lymphoedema describe the cumulative costs of practitioner fees,
compression garments and skin and wound care products.
• People with lymphoedema also report needing to take leave from work or having their
employment affected.
• More serious cases can result in long-term disability and unemployment.
• Hospital admissions for cellulitis requiring intravenous antibiotic therapy result in
substantial, and potentially avoidable, costs to the health care system. 37
Permanency & Early Intervention
The majority of the literature sourced suggests that lymphedema is permanent, and that treatment
focuses on reducing the swelling and control ing the pain.
“Lymphoedema is a chronic condition that is not curable at present, but may be al eviated by
appropriate management; if ignored, it can progress and become difficult to manage”. 38
Research indicates that early diagnosis and treatment intervention of lymphoedema allows
improved quality of life:
“Early diagnosis of lymphedema translates to more treatment options; less edema, smaller limbs,
improvement in joint aches, and reduced muscle pain and tightness; a decreased infection rate;
36 NSW Government, Agency for Clinical Innovation, "Lymphoedema: A guide for clinical services",
2018, p 4, https://www.aci.health.nsw.gov.au/ data/assets/pdf file/0008/477998/lymphoedema-
guide.pdf
37 NSW Government, Agency for Clinical Innovation, "Lymphoedema: A guide for clinical services",
2018, p 4, https://www.aci.health.nsw.gov.au/ data/assets/pdf file/0008/477998/lymphoedema-
guide.pdf
38 International Lymphoedema Framework, "International Consensus, Best Practice for the
Management of Lymphoedema", p. 2, 2006, https://www.lympho.org/wp-
content/uploads/2016/03/Best practice.pdf
Research Request - Oedema and Lymphoedema Management | Page 22 of 24
Page 22 of 24

FOI 23/24-1268
increased patient desire to continue treatment; decreased medical costs; and an improved quality of
life.” 39
The International Lymphoedema Framework, best practice guidelines suggest that:
“People at risk of lymphoedema should be identified early during routine assessment, monitored
and taught self care, and that patients and carers should have early active involvement in the
management of lymphoedema”. 40
“It is our goal to prevent lymphoedema occurring or at least detect it early to avoid long term
problems. Prevention and early detection are the keys to success and there are things that can be
done to help reduce the risk”. 41
Reference List
A. Soran et al., "Lymphedema Prevention and Early Intervention: A Worthy Goal", MJH Life
Sciences, Vol 26, No 3, 2012, https://www.cancernetwork.com/articles/lymphedema-prevention-
and-early-intervention-worthy-goal
Australasian Lymphology Association, "Training in Lymphoedema Management", [website], 2020,
https://www.lymphoedema.org.au/the-register/lymphoedema-training-courses, (accessed 6
January 2020)
Australasian Lymphology Association, "What is Lymphoedema?" [website], 2020,
https://www.lymphoedema.org.au/about-lymphoedema/what-is-lymphoedema, (accessed 8
January 2020)
Australasian Lymphology Association, "Position Statement: The Use of Compression Garments In
the Management of Lymphoedema", 2012,
https://www.lymphoedema.org.au/public/7/files/Position%20Statements/ALA%20Poistion%20St
atement%20on%20Compression%20Garments.pdf
Better Health Channel, "Fluid retention (oedema)", [website] 2018,
https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/Fluid-retention-oedema,
(accessed 7 January 2020)
39 A. Soran et al., "Lymphedema Prevention and Early Intervention: A Worthy Goal", MJH Life
Sciences, Vol 26, No 3, 2012, https://www.cancernetwork.com/articles/lymphedema-prevention-
and-early-intervention-worthy-goal
40 International Lymphoedema Framework, "International Consensus, Best Practice for the
Management of Lymphoedema", 2006, https://www.lympho.org/wp-
content/uploads/2016/03/Best practice.pdf
41 Westmead Breast Cancer Institute., "Fact Sheet: Lymphedema", [website], 2014,
https://www.bci.org.au/breast-cancer-information/fact-sheets/lymphoedema, (accessed 10 January
2020)
Research Request - Oedema and Lymphoedema Management | Page 23 of 24
Page 23 of 24

FOI 23/24-1268
D. Tidhar et al., "Aqua Lymphatic Therapy in Managing Lower Extremity Lymphedema", J Support
Oncol, Vol 5, pp. 179-183, 2007, http://www.aqua-lymphatic-
therapy.com/files/Aqua Lymphatic Therapy in Managing Lower Extremity Lymphedema.pdf
Hand Therapy Group, "Lymphedema and Oedema: What’s the difference?", [website], 2016,
http://handtherapy.com.au/lymphedema-and-oedema-whats-the-difference, (accessed 6 January
2020
International Lymphoedema Framework, "International Consensus, Best Practice for the
Management of Lymphoedema", 2006, https://www.lympho.org/wp-
content/uploads/2016/03/Best practice.pdf
Lymphoedema Action Alliance, Submission to The Standing Committee on Health: Inquiry into
Chronic Disease Prevention and Management in Primary Health Care (Submission on the
prevention and management of Lymphoedema in Primary Health Care, 2015,
https://www.cancercouncil.com.au/wp-content/uploads/2016/01/CCNSW-Submission Inquiry-
into-chronic-disease-prevention-and-mgmt-of-lymphoedema-in-primary-health-
care_Lymphoedema-Action-Alliance_July-2015.pdf
Mayo Clinic, "Oedema", [website] 2020, https://www.mayoclinic.org/diseases-
conditions/edema/symptoms-causes/syc-20366493, (accessed 7 January 2020)
Medical News Today, "What is dependent edema?", [website], 2020,
https://www.medicalnewstoday.com/articles/320986.php, (accessed 10 January 2020)
NHS, Causes: Lymphoedema, [website], 2019,
https://www.nhs.uk/conditions/lymphoedema/causes, (accessed 06 January 2020)
NSW Government, Agency for Clinical Innovation, "Lymphoedema:
A guide for clinical services", 2018,
https://www.aci.health.nsw.gov.au/ data/assets/pdf file/0008/477998/lymphoedema-
guide.pdf
P. Baker, "Is there a role for contrast Hydrotherapy", Journal of Lymphoedema, Vol 6, No 2, 2011,
https://www.woundsinternational.com/uploads/resources/content 11212.pdf
S. Ehmann and K. Bock, "Functionality to measure outcomes for safety, effectiveness and cost
implications" (New Frontiers in Wound Management New Frontiers in Wound AND Edema
Management, EWMA), 2018, https://ewma.org
The Lymphie Life "Lymphedema vs Edema", [website], 2012,
https://thelymphielife.com/2012/03/31/lymphedema-vs-edema, (accessed 6 January 2020)
Westmead Breast Cancer Institute., "Fact Sheet: Lymphedema", [website], 2014,
https://www.bci.org.au/breast-cancer-information/fact-sheets/lymphoedema, (accessed 10
January 2020)
Your.MD, "Oedema", [website] 2020, https://www.your.md/condition/oedema, (accessed 7
January 2020)
Research Request - Oedema and Lymphoedema Management | Page 24 of 24
Page 24 of 24