DOCUMENT 3
DOCUMENT 3
FOI 24/25 - 0189
Research Request – Respiratory Support Practice Guidance
I am requesting some assistance from our research team for developing the Respiratory
practice guidance.
Tracheostomy supports:
• Clinical guidelines for tracheostomy indications and care – change of
tracheostomy and regular maintenance care
• Referring/monitoring health professionals – e.g. Respiratory Specialist of GP
• Evidence that this support is directly related to any specific disabilities (e.g. spinal
cord injury above C3 level)
• Typical equipment required
Constant Positive Airway Pressure (CPAP)
Brief
• Clinical guidelines for CPAP use and indications
• Referring/monitoring professionals – e.g. Respiratory Specialist of GP
• Evidence that support is directly related to any specific disabilities (assist in
sleeping and breathing for people with compromised breathing function as a
result of their disability).
• Typical equipment and consumables (such as mask, head straps and tubes)
Same for:
• Bilevel Positive Airway Pressure (BIPAP)
• Air Humidifier
• Cough assist machine
• Suction machine
Date
26/08/19
Requester
Karyn s47F - personal
priva
Craig
(
s47F - personal Tactical Research Advisor – TAT)
Researchers Aanika s47F - personal p(Senior Research Officer – TAT)
P a g e |
1
Page 1 of 21

FOI 24/25 - 0189
Contents
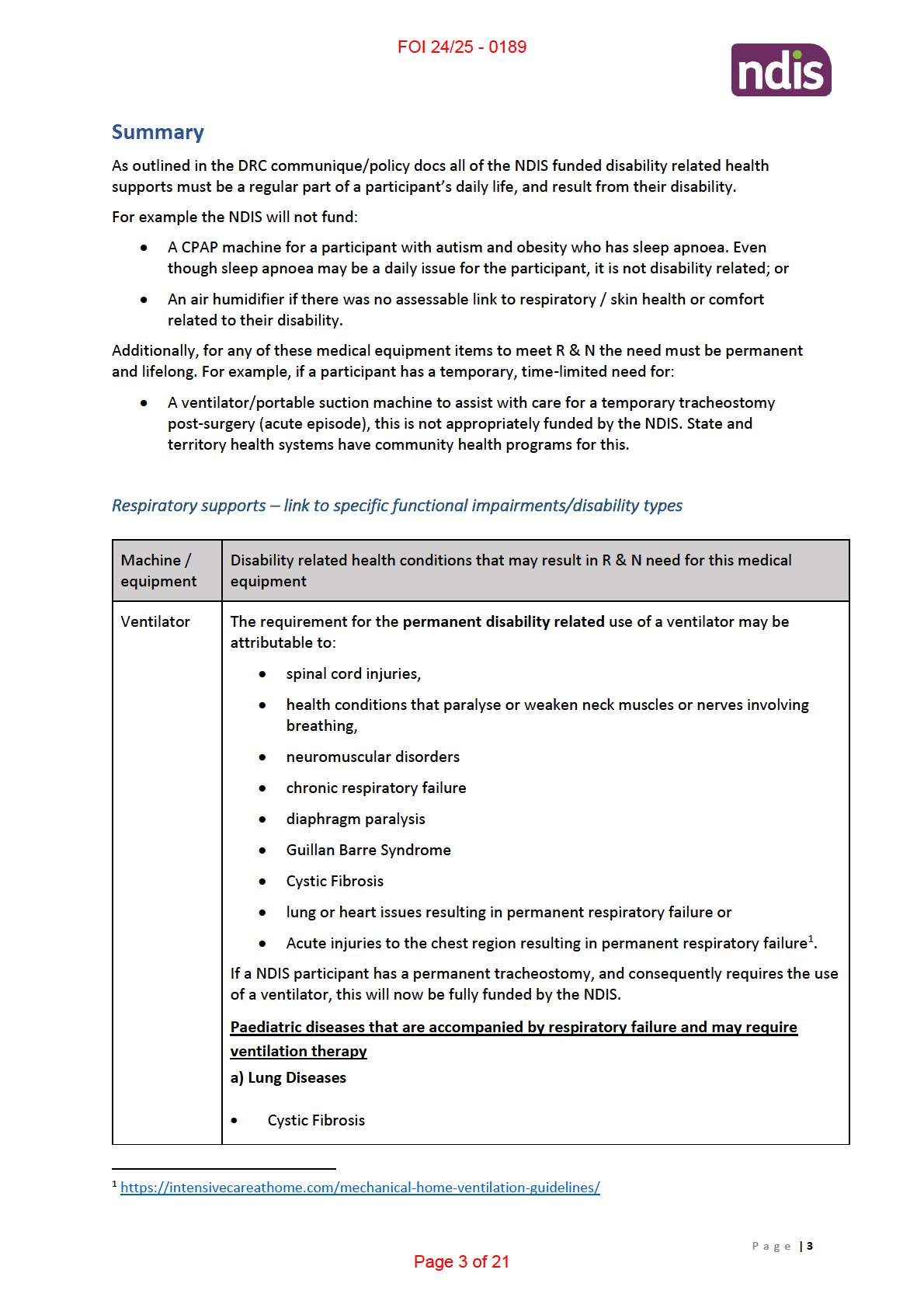
Summary ................................................................................................................................................. 3
Respiratory supports – link to specific functional impairments/disability types ........................... 3
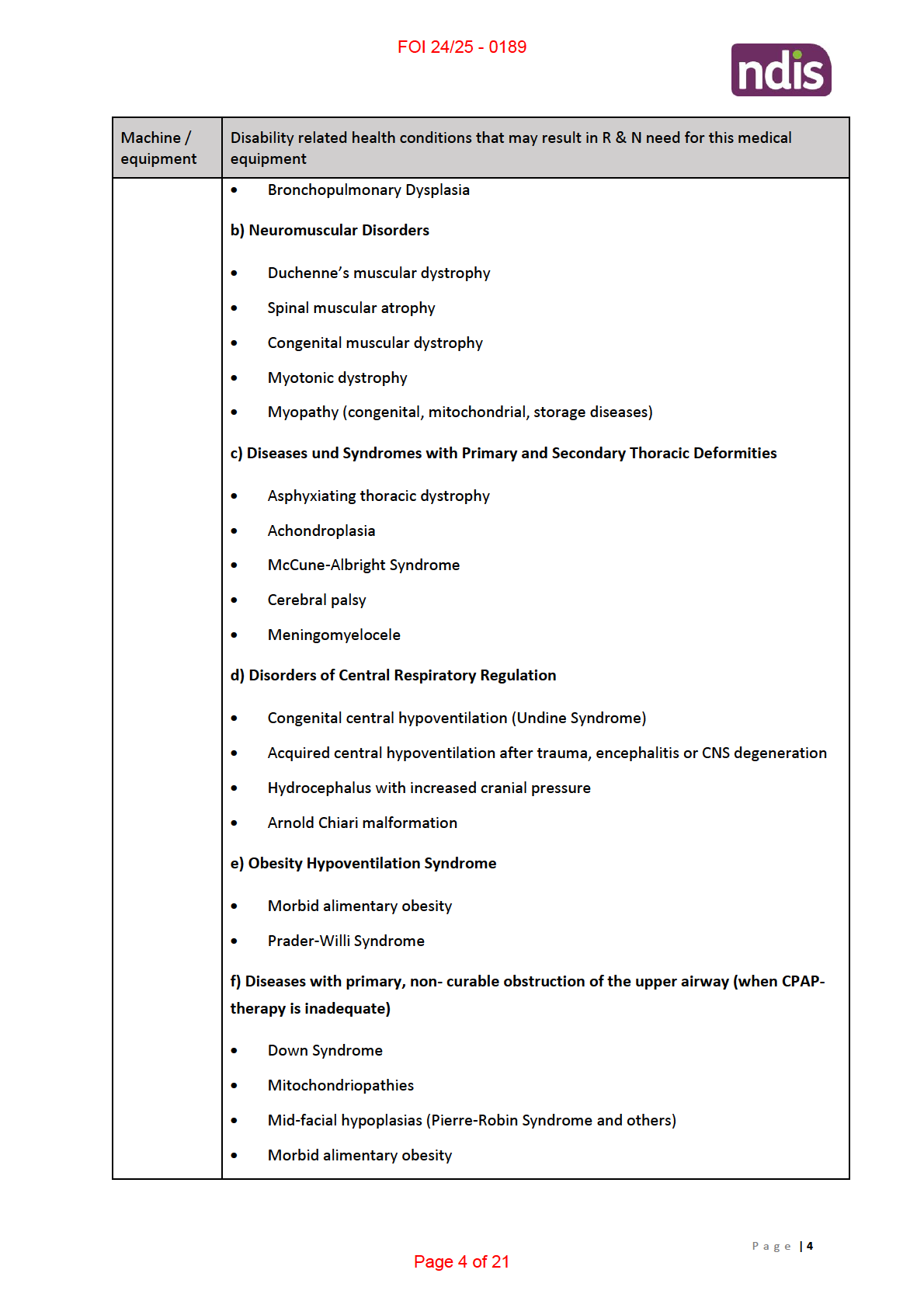
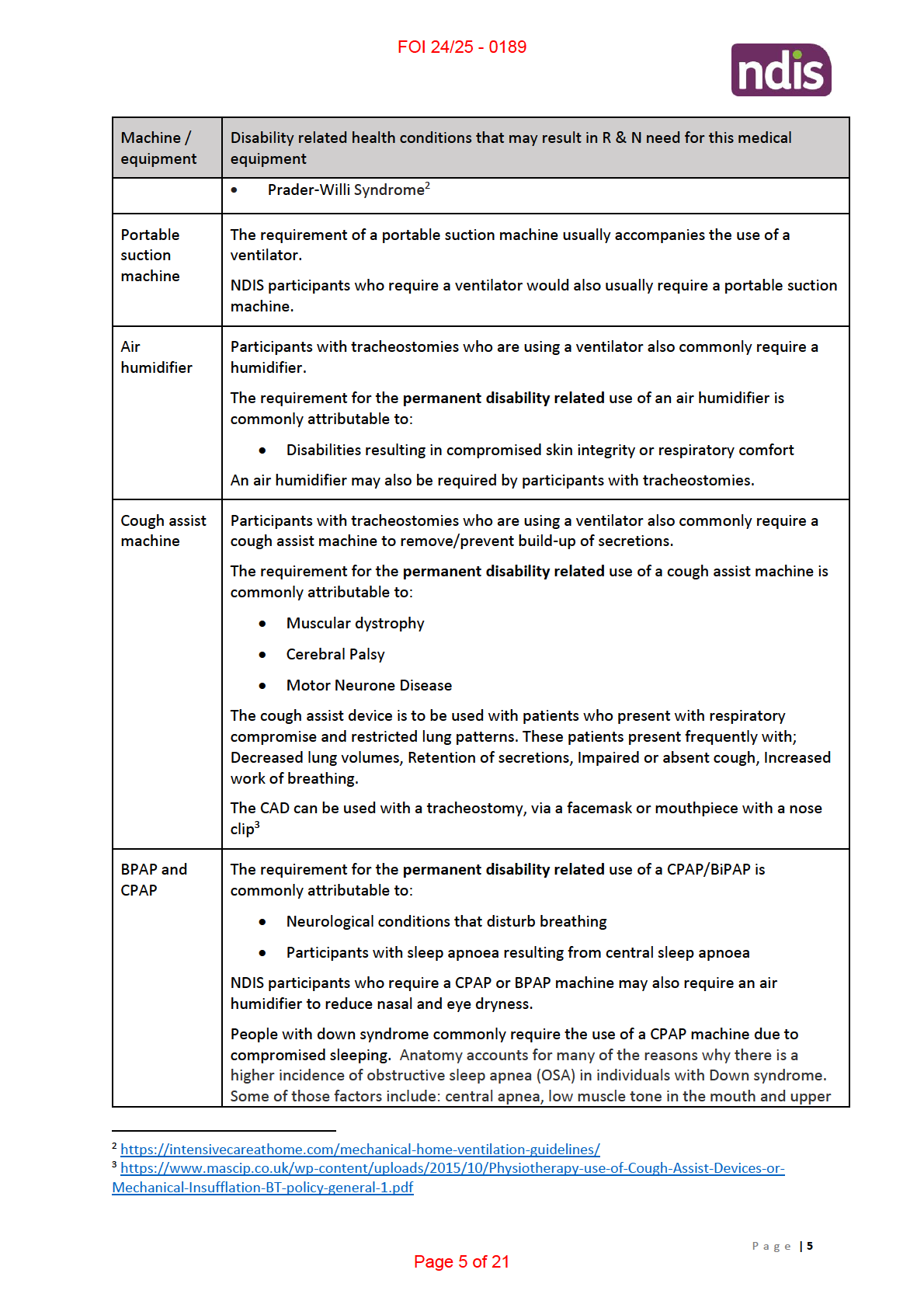
Paediatric diseases that are accompanied by respiratory failure and may require ventilation
therapy............................................................................................................................................ 3
Tracheostomy ......................................................................................................................................... 6
➢ Clinical guidelines for indication and use .................................................................................... 6
➢ Referring/prescription and monitoring by health professionals? .............................................. 7
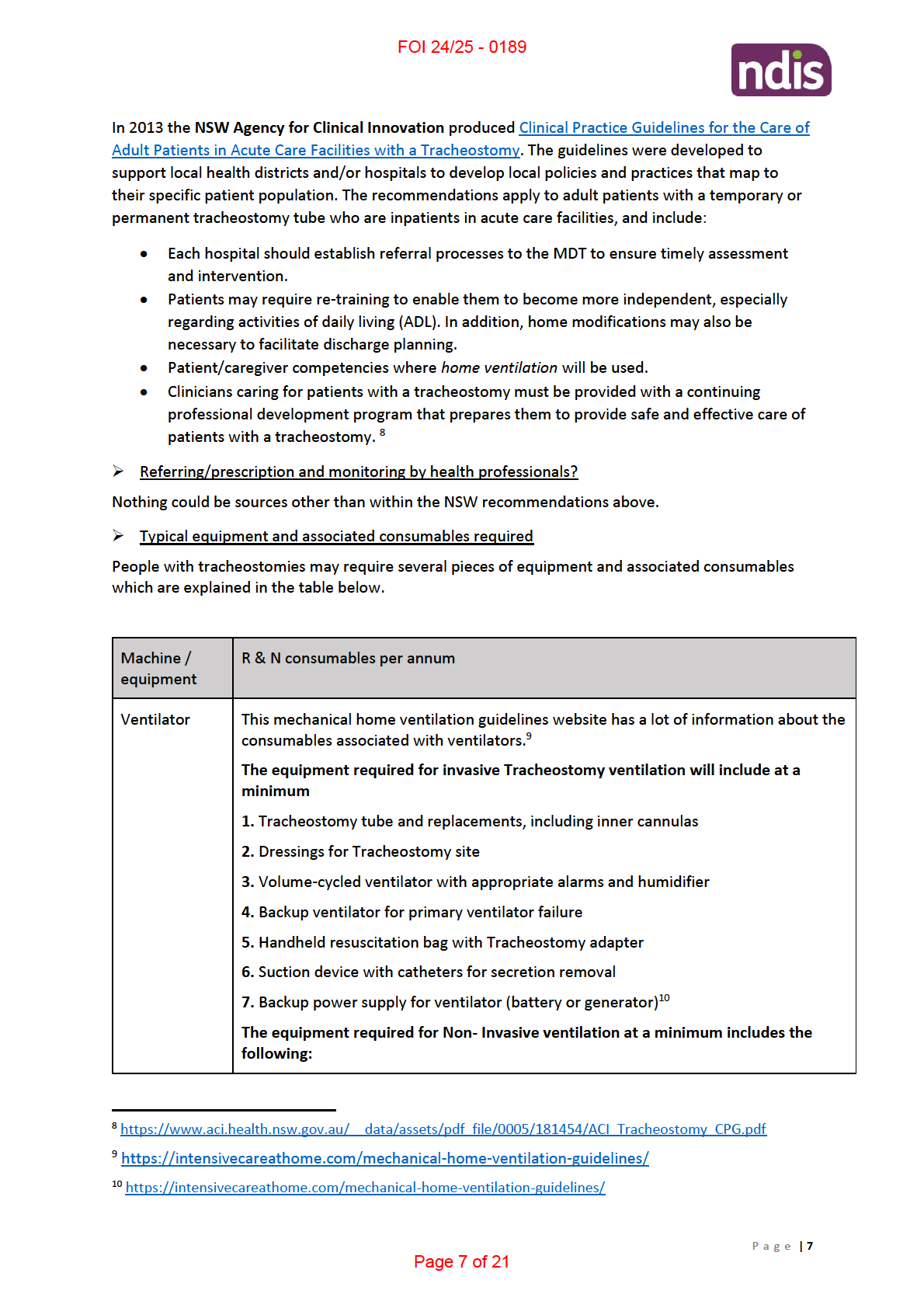
➢ Typical equipment and associated consumables required ......................................................... 7
Suction Machine ..................................................................................................................................... 8
➢ Clinical guidelines for indication and use .................................................................................... 8
➢ Referring/prescription and monitoring by health professionals? .............................................. 9
➢ Typical equipment and consumables required ........................................................................... 9
Air Humidifier .......................................................................................................................................... 9
➢ Clinical guidelines for indication and use .................................................................................... 9
➢ Referring/prescription and monitoring by health professionals? ............................................ 10
➢ Evidence that this support is linked with any specific disabilities? .......................................... 10
➢ Typical equipment and consumables required ......................................................................... 10
Cough Assist Machine ........................................................................................................................... 10
➢ Clinical guidelines for indication and use .................................................................................. 10
➢ Referring/prescription and monitoring by health professionals? ............................................ 11
➢ Evidence that this support is linked with any specific disabilities? .......................................... 11
➢ Typical equipment and consumables required ......................................................................... 11
CPAP ...................................................................................................................................................... 12
➢ Clinical guidelines for indication and use .................................................................................. 12
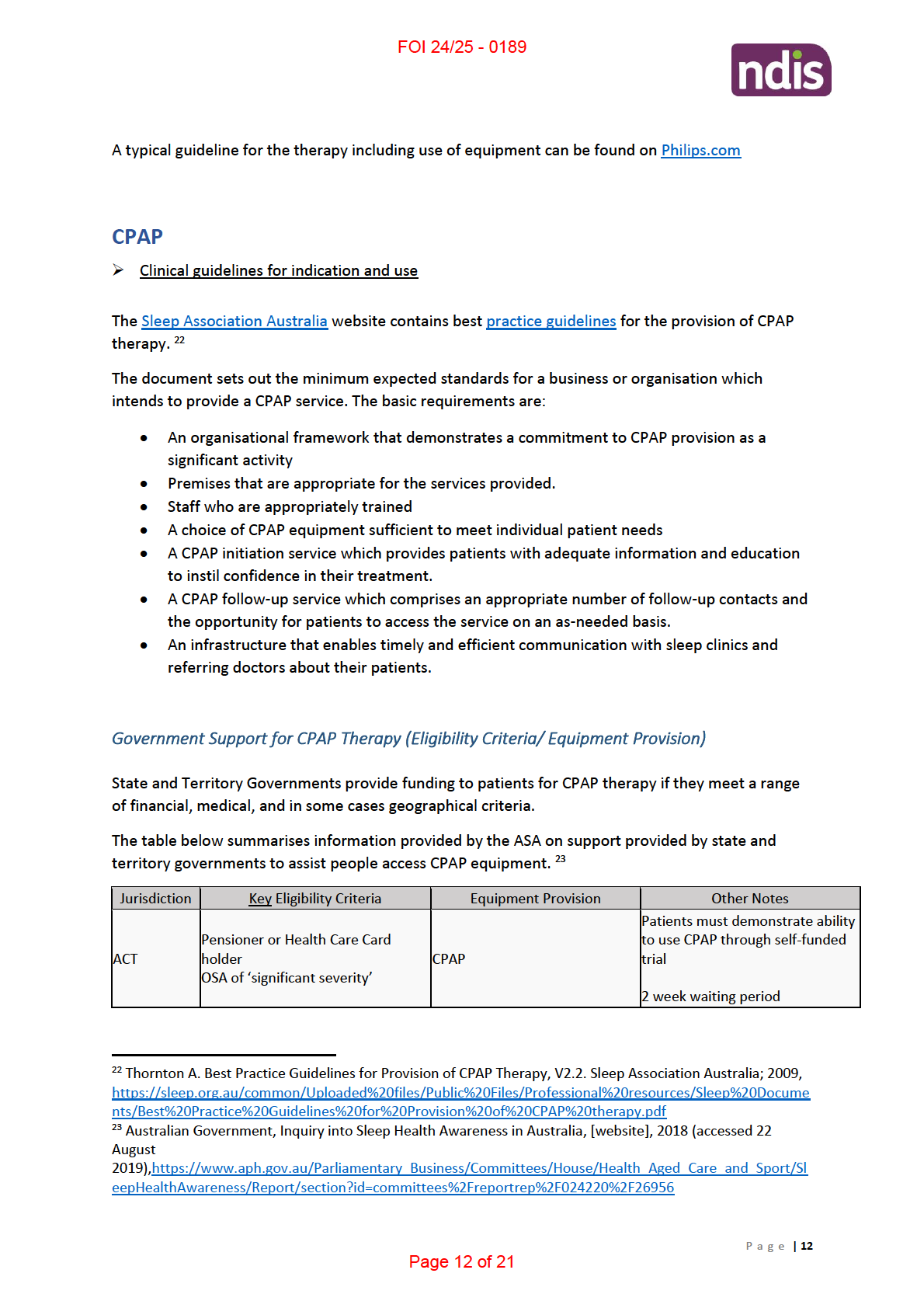
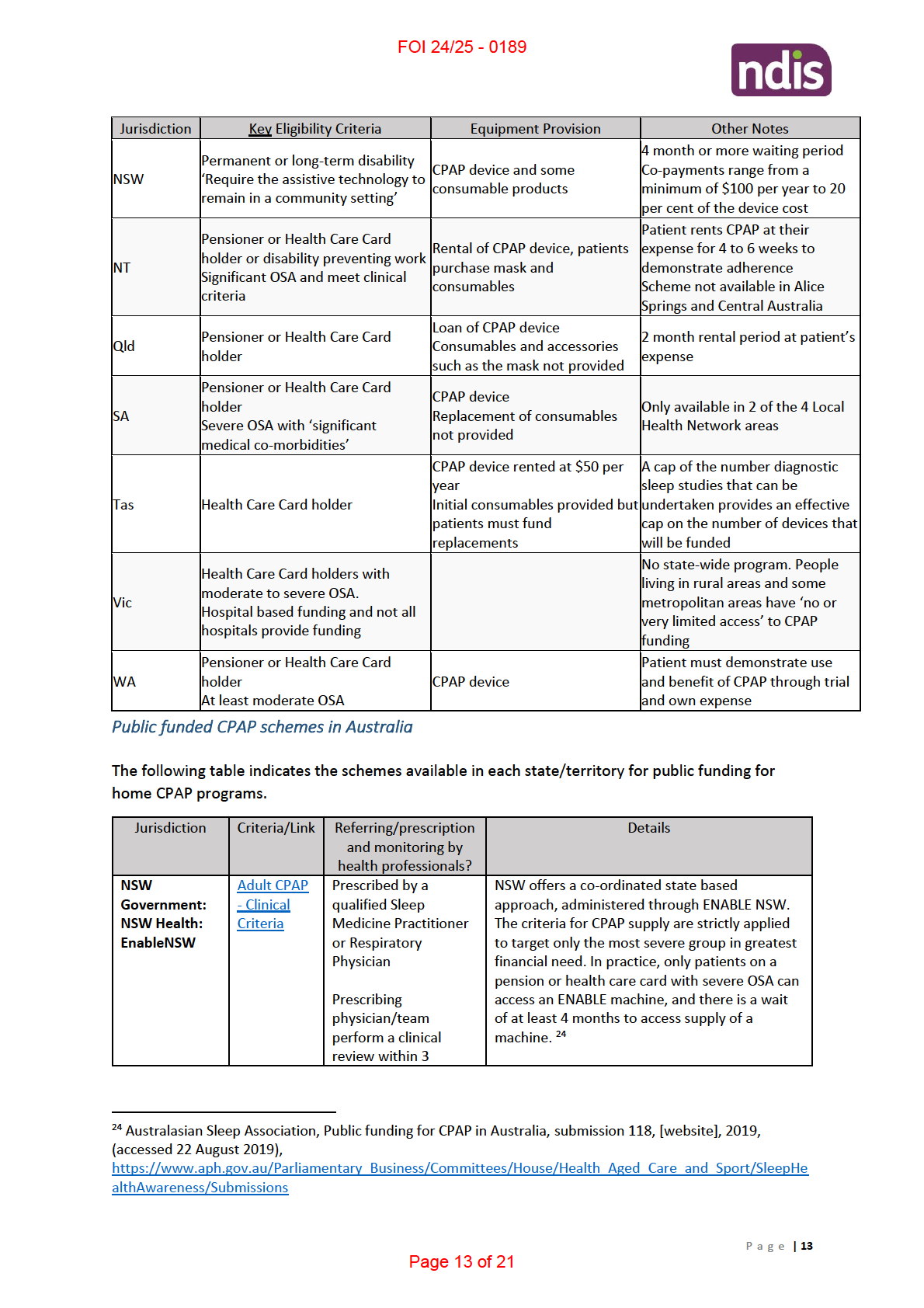
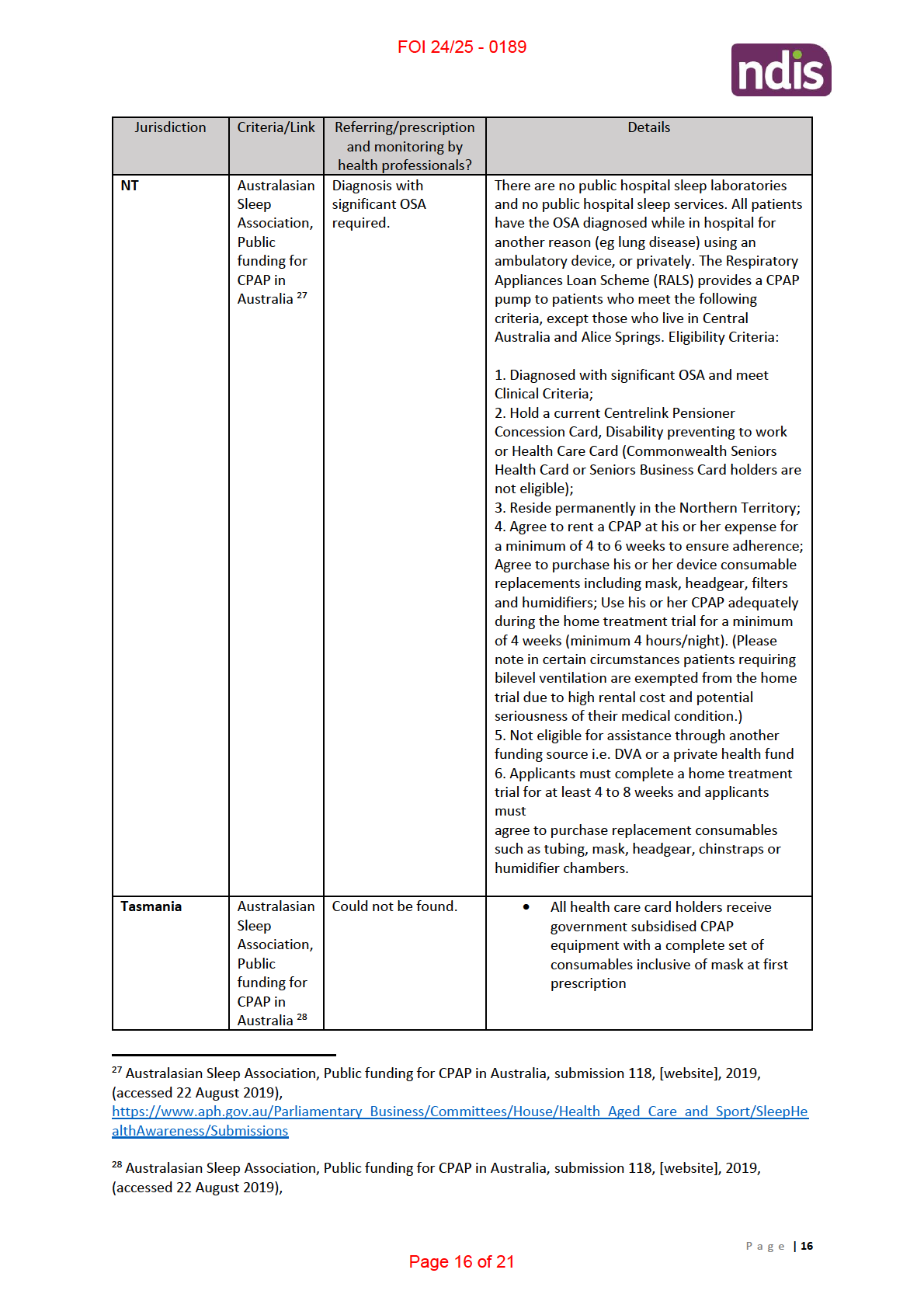
Government Support for CPAP Therapy (Eligibility Criteria/ Equipment Provision) .................... 12
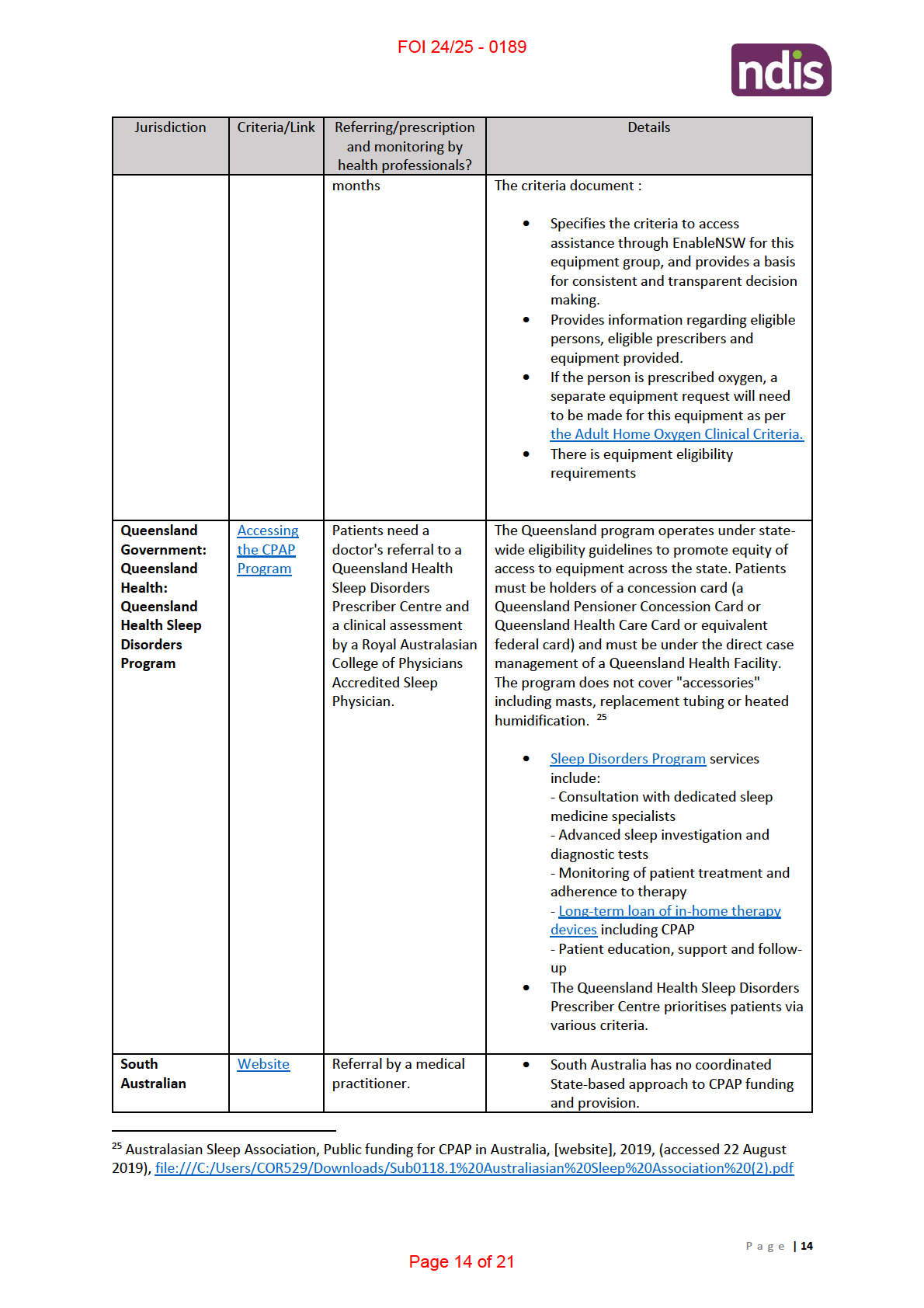
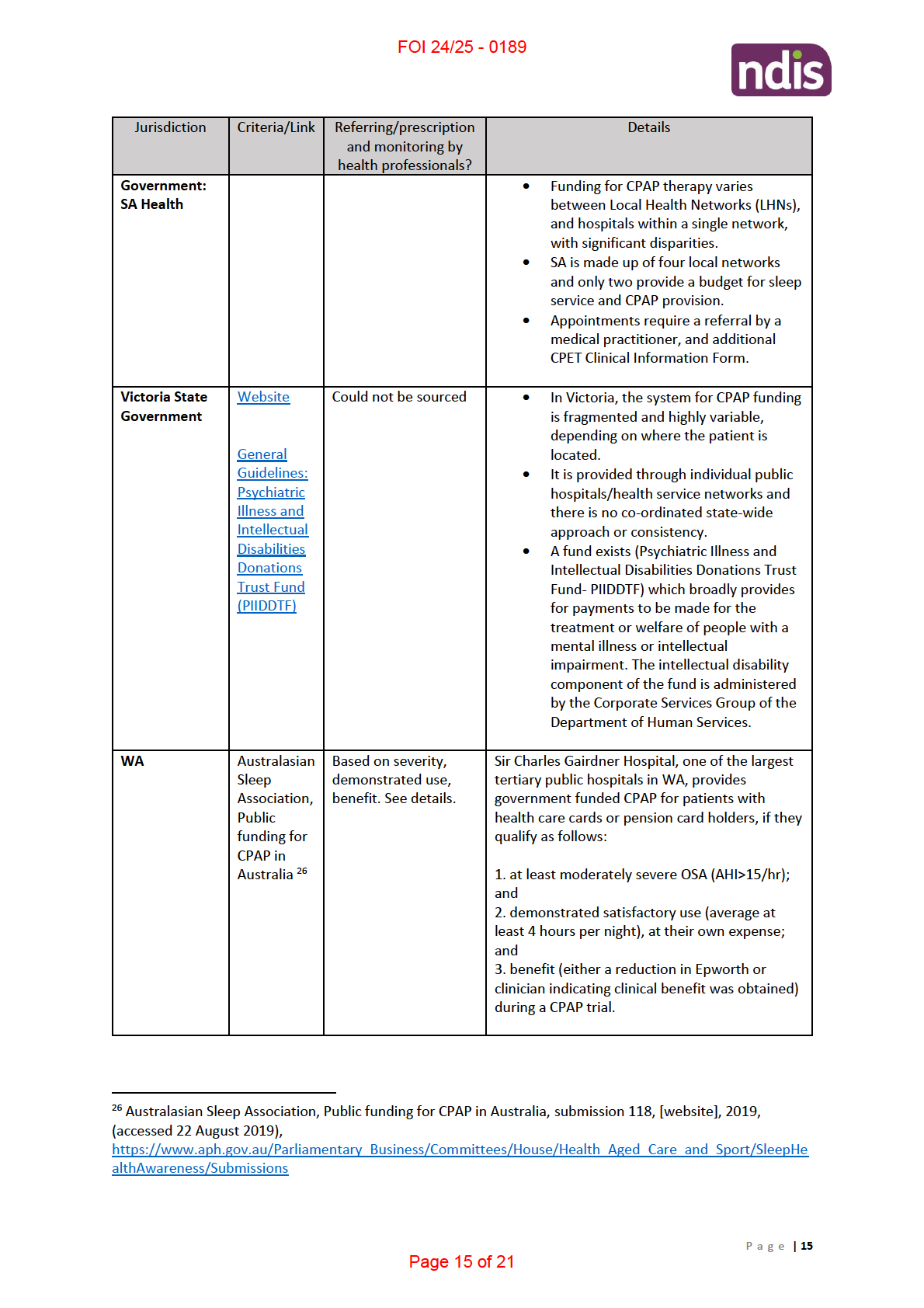
Public funded CPAP schemes in Australia ..................................................................................... 13
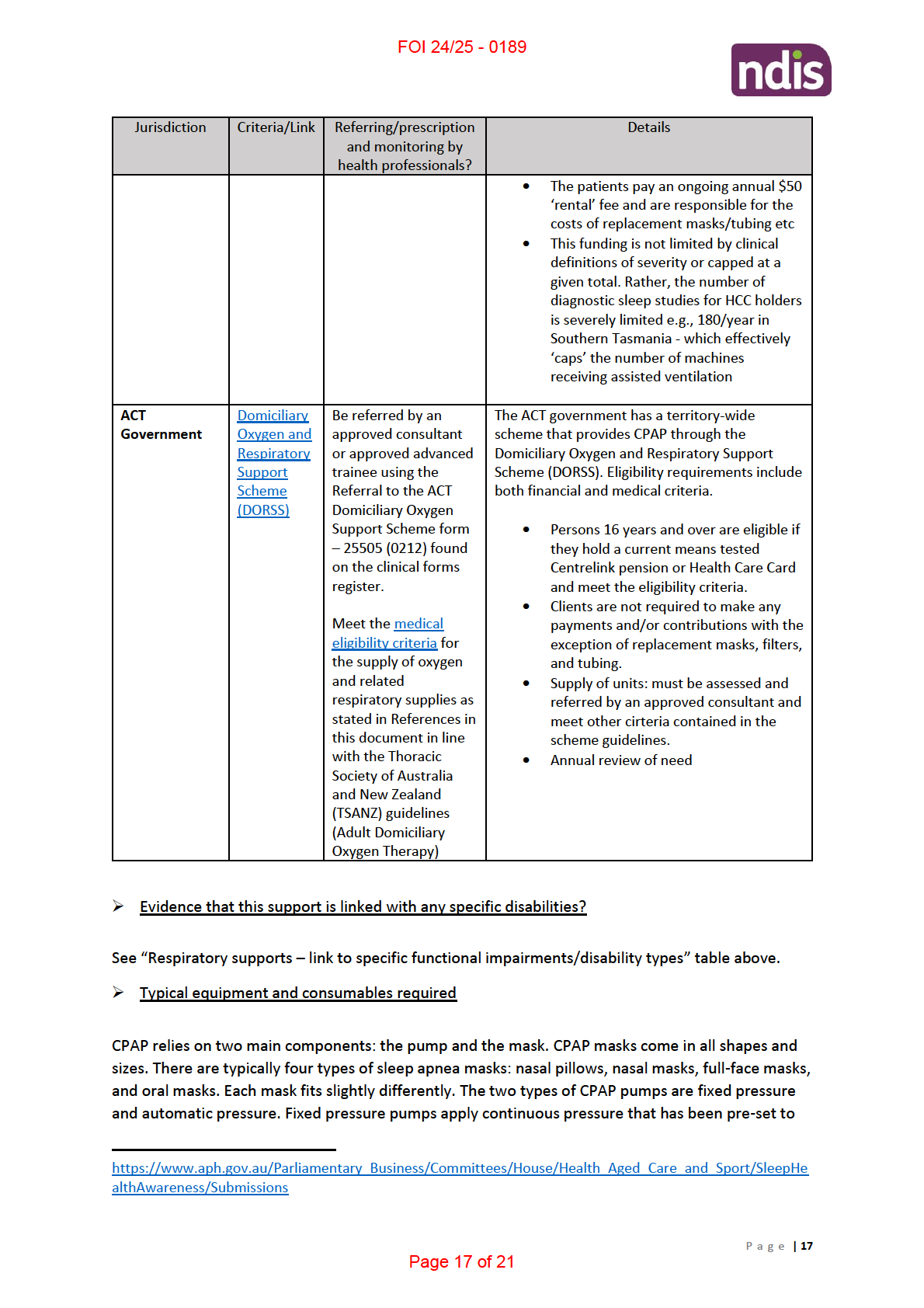
➢ Evidence that this support is linked with any specific disabilities? .......................................... 17
➢ Typical equipment and consumables required ......................................................................... 17
BIPAP ..................................................................................................................................................... 18
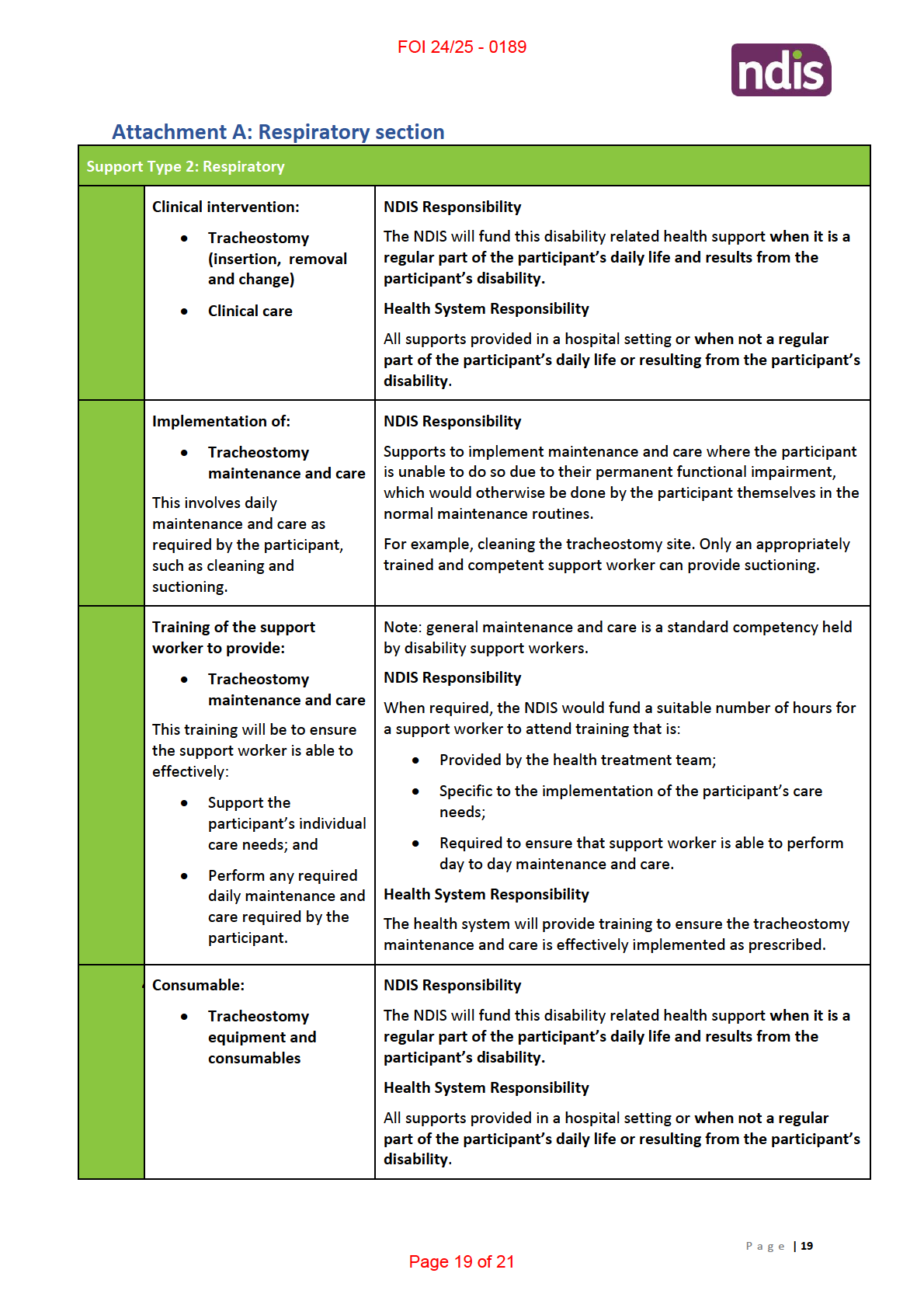
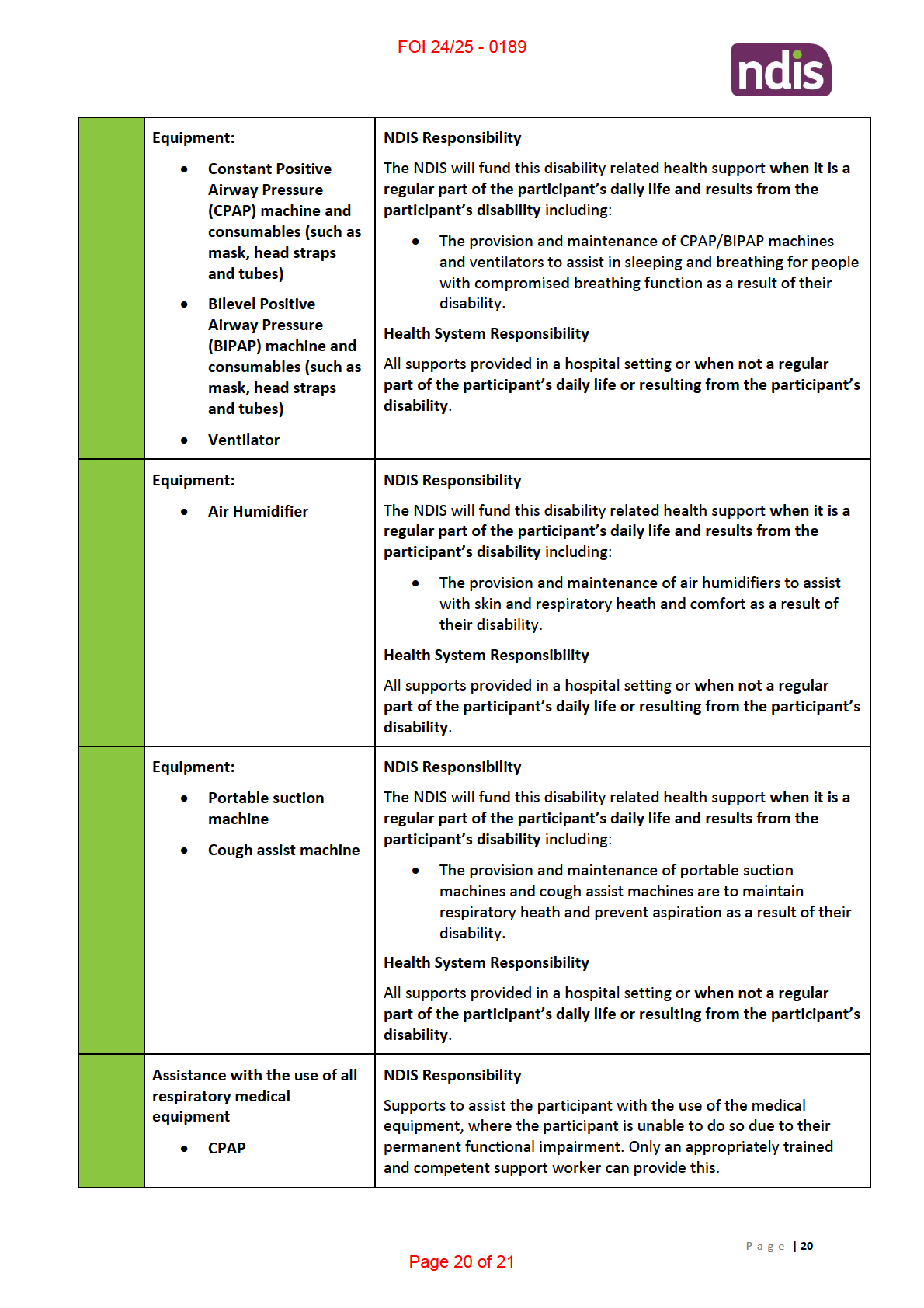
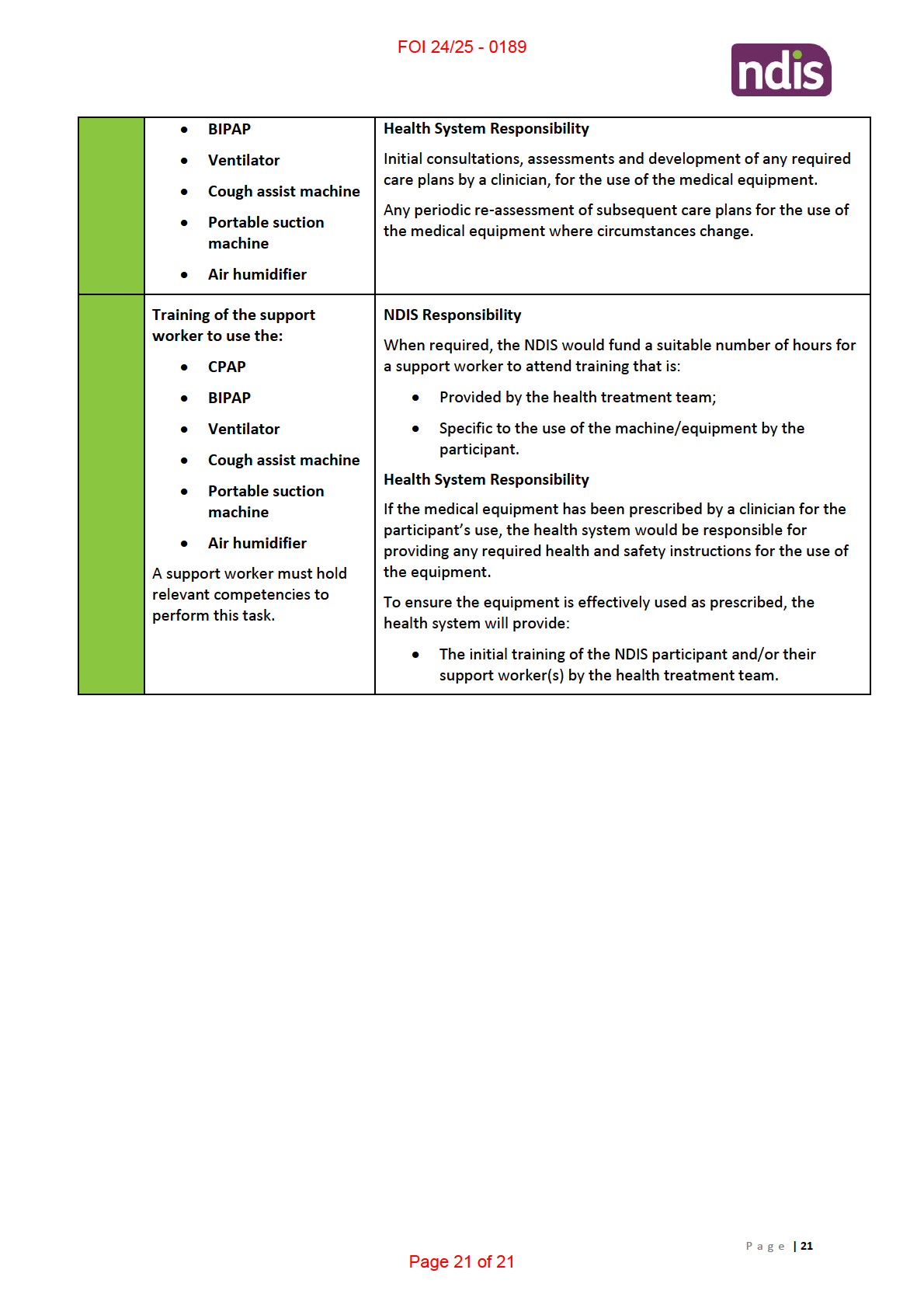
Attachment A: Respiratory section ....................................................................................................... 19
P a g e |
2
Page 2 of 21

FOI 24/25 - 0189
1. Pressure- or volume-type ventilator
2. Appropriate interface mask or mouthpiece
3. Secretion management program or device
4. Backup power supply for ventilator (battery or generator)
Suction Machine
Endotracheal suctioning (ETS) is one of the most common procedures performed in patients with
artificial airways. It is a component of bronchial hygiene therapy and mechanical ventilation that
involves the mechanical aspiration of pulmonary secretions from a patient’s artificial airway to
prevent its obstruction. The procedure includes patient preparation, the suctioning event, and
follow-up care.
There are two (2) methods of endotracheal suctioning based on the selection of catheter: open and
closed. The open suctioning technique requires disconnecting the patient from the ventilator, while
the closed suctioning technique involves attachment of a sterile, closed, in-line suction catheter to
the ventilator circuit, which allows passage of a suction catheter through the artificial airway without
disconnecting the patient from the ventilator.
There are also two (2) methods of suctioning based on the catheter suction depth selected during
the procedure: deep and shallow. Deep suctioning is defined as the insertion of a suction catheter
until resistance is met, followed by withdrawal of the catheter by 1 cm before application of
negative pressure, and shallow suctioning as the insertion of a suction catheter to a predetermined
depth, usually the length of the artificial airway plus the adapter11.
This journal article also provides information about the setting that suctions may be performed
(Hospital, Extended care facility, Home, Out-patient clinic, Physician’s office, Transport vehicle)12.
It also provides information on associated care, monitoring, assessment of need, assessment of
outcomes and the actual procedure.
➢ Clinical guidelines for indication and use
A journal article from 2010 by the American Association for Respiratory Care examining
endotracheal suctioning of mechanically ventilated patients with artificial airways concludes that:
(1) It is recommended that endotracheal suctioning should be performed only when
secretions are present, and not routinely;
(2) It is suggested that pre-oxygenation be considered if the patient has a clinically important
reduction in oxygen saturation with suctioning;
(3) Performing suctioning without disconnecting the patient from the ventilator is suggested;
(4) Use of shallow suction is suggested instead of deep suction, based on evidence from
infant and pediatric studies;
11 https://www.aarc.org/wp-content/uploads/2014/08/06.10.0758.pdf
12 Page 759.
P a g e |
8
Page 8 of 21

FOI 24/25 - 0189
(5) It is suggested that routine use of normal saline instillation prior to endotracheal suction
should not be performed;
(6) The use of closed suction is suggested for adults with high FIO2, or PEEP, or at risk for
lung derecruitment, and for neonates;
(7)Endotracheal suctioning without disconnection (closed system) is suggested in neonates;
(8) Avoidance of disconnection and use of lung recruitment maneuvers are suggested if
suctioning-induced lung derecruitment occurs in patients with acute lung injury;
(9) It is suggested that a suction catheter is used that occludes less than 50% the lumen of
the endotracheal tube in children and adults, and less than 70% in infants;
(10) It is suggested that the duration of the suctioning event be limited to less than 15
seconds 13.
A clinical guideline has been developed by Intensive Care NSW, to provide clinicians with
recommendations to guide the development of local policy/procedures in related to suction through
an artificial airway in critically ill adult patients in NSW acute care facilities. 14
➢ Referring/prescription and monitoring by health professionals?
No information could be sourced.
➢ Typical equipment and consumables required
This information is covered off in the tracheostomy table above. Most participants with a ventilator
will also require suctioning.
Air Humidifier
➢ Clinical guidelines for indication and use
A journal article from 2012 by the American Association for Respiratory Care investigating
humidification during invasive and non-invasive mechanical ventilation provides the following
information:
• When the upper airway is bypassed during invasive mechanical ventilation, humidification is
necessary to prevent hypothermia, disruption of the airway epithelium, bronchospasm,
atelectasis, and airway obstruction. In severe cases, inspissation of airway secretions may
cause occlusion of the endotracheal tube.1 While there is not clear consensus on whether or
not additional heat and humidity are always necessary when the upper airway is not
bypassed, such as in non-invasive mechanical ventilation (NIV), active humidification is
highly suggested to improve comfort.2-7 Two systems, active humidification through a
13 Page 758 https://www.aarc.org/wp-content/uploads/2014/08/06.10.0758.pdf
14 https://www.aci.health.nsw.gov.au/networks/icnsw/intensive-care-manual/statewide-
guidelines/suctioning-an-adult-icu-patient
P a g e |
9
Page 9 of 21

FOI 24/25 - 0189
heated humidifier (HH) and passive humidification through a heat and moisture exchanger
(HME), are available for warming and humidifying gases delivered to mechanically ventilated
patients. There are 3 types of HME or artificial nose: hydrophobic, hygroscopic, and a filtered
HME15.
• Humidification is recommended on every patient receiving invasive mechanical ventilation.
Active humidification is suggested for NIV, as it may improve adherence and comfort 16
➢ Referring/prescription and monitoring by health professionals?
No information could be sourced.
➢ Evidence that this support is linked with any specific disabilities?
See “Respiratory supports – link to specific functional impairments/disability types” table above.
➢ Typical equipment and consumables required
The basic parts of a humidifier:
• Water Control Valve (Float): Allows the humidifier to receive water flow
• Fan: The fan assists the evaporation of the water by blowing air into the wick. (Not in all
humidifiers)
• Reservoir: The reservoir holds the water, which is needed to produce evaporation.
Other components that are needed for a humidifier to operate, but are not in all types, are:
• Wick (Filter)
• Evaporator Pad
• Heating Element 17
Cough Assist Machine
Cough assist machines are also referred to as Mechanical Insufflation-Exsufflation. Mechanical
Insufflation-Exsufflation (MIE) or a Cough Assist Device (CAD) is the use of positive airway pressure
which rapidly changes to negative pressure to assist the patient’s cough. Patients for a wide variety
of reasons and conditions are unable to cough or clear airway secretions effectively due to reduced
peak cough flow. These devices assist in the mobilisation and clearance of bronchial secretions by
inflating the lungs. MIE is an alternative to suctioning providing decreased mucosal trauma and
increased patient comfort18.
➢ Clinical guidelines for indication and use
A 2019 policy guideline for Derby & Derbyshire in the UK, states: “
There is currently insufficient
evidence to support the use of Mechanical Insufflation-exsufflation (MI-E) for patients with neuron
15 Restrepo, RD & Walsh BK, ‘Humidification During Invasive and Noninvasive Mechanical Ventilation: 2012’,
American Association for Respiratory Care,
Respiratory Care, May 2010 Vol 57 No 5, Page 782
<http://www.rcjournal.com/cpgs/pdf/12.05.0782.pdf> accessed 23 August 2019.
16 Page 786 http://www.rcjournal.com/cpgs/pdf/12.05.0782.pdf
17 http://www.lumacomfort.com/article/how-your-humidifier-works.htm
18 https://www.mascip.co.uk/wp-content/uploads/2015/10/Physiotherapy-use-of-Cough-Assist-Devices-or-
Mechanical-Insufflation-BT-policy-general-1.pdf
P a g e |
10
Page 10 of 21

FOI 24/25 - 0189
muscular dystrophy (NMD) or spinal cord problems. Derby and Derbyshire CCG therefore do not
routinely fund MI-E.
Guidance from a range of professional bodies has supported its use, based on low quality evidence or
expert opinion. Further research is needed to establish the effects relating to reducing infections,
safety, its use in the longer term and its cost effectiveness. Some of this has started to be addressed
at a national and international level but will take some time to be available.
There may be exceptional circumstances where a clinician can demonstrate that a patient can derive
significantly greater benefit from the technology than other patients. In these circumstances please
read the Individual Funding Request (IFR) policy and complete the relevant form.
This policy statement applies to both children and adults”. 19
➢ Referring/prescription and monitoring by health professionals?
No information could be sourced. No public schemes/programs could be found in Australia other
than a Cough Assist Program administered by Spinal Muscular Atrophy Australia Inc. This is a
members loaning scheme, with a pool of 15 CA-3200 and 10 E-70 Cough Assist Machines. The
criteria for loan is:
• Any person/family requesting to use a machine MUST be a member of Spinal Muscular
Atrophy Australia Inc.
• Any person/family requesting a machine must complete an Application for Equipment Form
• A letter from a Respiratory Specialist must accompany the application. The letter must state;
i) The name of person using machine.
ii) The machine will be of benefit to that person.
iii) That the person/family has been trained and can appropriately use the machine.
➢ Evidence that this support is linked with any specific disabilities?
See “Respiratory supports – link to specific functional impairments/disability types” table above.
➢ Typical equipment and consumables required
Cough Assist equipment would typically be the machine and a mask. 20There are various products on
the market.
New assisted cough machines are small, lighter, and convenient for home and travel. The
mechanically assisted cough, or cough assist machine uses a facemask, mouthpiece, or tracheostomy
to deliver gradual positive air pressure to the airway. 21
19 http://www.derbyshiremedicinesmanagement.nhs.uk/assets/clinical-
policies/clinical policies/other/cough assist policy.pdf
20http://incenter.medical.philips.com/doclib/enc/9984488/CAT70_Quick_start.pdf%3ffunc%3ddoc.Fetch%26n
odeid%3d9984488
21 https://www.parentprojectmd.org/care/care-guidelines/by-area/care-for-lung-muscles/assistive-devices-
for-coughing/
P a g e |
11
Page 11 of 21

FOI 24/25 - 0189
suit your specific requirements. Automatic pressure pumps monitor airflow and continuously adjust
air pressure based on changing needs throughout the night. These kinds of pumps are most useful
for patients whose positive airway pressure requirements vary during sleep. 29
Various equipment associated with CPAP:
CPAP MACHINES: Fixed Pressure, Automatic Variable Pressure, Travel CPAP Machines,
CPAP MASKS: Nasal Pillow, Nasal, Full Face, CPAP Mask Parts (Various)
CPAP ACCESSORIES: Battery Kits, Tubing, Humidifier, Filters, Power, Cleaning, Chin Straps, Lumin -
CPAP Sanitiser
BIPAP
BIPAP is comparable to CPAP.
29
CPAP Australia, What is CPAP? Everything you need to know, [website], 2019, (accessed August 22 2019),
https://ww2.cpapaustralia.com.au/blog/what-is-cpap
P a g e |
18
Page 18 of 21