FOI 24/25- 0013
DOCUMENT 36
Thermoregulation and air conditioning
The content of this document is OFFICIAL.
Please note:
The research and literature reviews collated by our TAB Research Team are not to be shared
external to the Branch. These are for internal TAB use only and are intended to assist our
advisors with their reasonable and necessary decision-making.
Delegates have access to a wide variety of comprehensive guidance material. If Delegates
require further information on access or planning matters, they are to call the TAPS line for
advice.
The Research Team are unable to ensure that the information listed below provides an
accurate & up-to-date snapshot of these matters
Research question: What medical conditions or disabilities involve an impairment in thermoregulation?
What cooling systems are available for use in Australia?
Is air conditioning effective in managing symptoms of thermoregulation impairment
compared to other cooling systems?
Date: 8/2/2024
Requestor: Helen s22(1)(a)(ii) - irrelevant material
Endorsed by: Melinda s22(1)(a)(ii) - irrelevant ma
Researcher: Aaron s22(1)(a)(ii)
- irrelevant ma
Cleared by: Stephanie s22(1)(a)(ii) - irrelevant mat
Page 391 of 425
FOI 24/25- 0013
1. Contents
Thermoregulation and air conditioning ....................................................................................... 1
1.
Contents ....................................................................................................................... 2
2.
Summary ...................................................................................................................... 3
3.
Human thermoregulation .............................................................................................. 4
3.1 Thermoeffectors ........................................................................................................ 4
4.
Conditions resulting in thermoregulation impairment .................................................... 5
4.1 Spinal cord injury ....................................................................................................... 7
4.2 Acquired brain injury .................................................................................................. 7
4.3 Parkinson’s Disease .................................................................................................. 8
4.4 Multiple Sclerosis ....................................................................................................... 8
4.5 Peripheral neuropathy ............................................................................................... 9
4.6 Psychosocial conditions ............................................................................................. 9
4.7 Epilepsy and seizure disorders ................................................................................ 10
4.8 Autism ...................................................................................................................... 10
4.9 Motor neurone disease / Amyotrophic lateral sclerosis............................................ 11
4.10 Huntington’s disease ............................................................................................ 11
4.11 Severe burns ........................................................................................................ 12
5.
Management of thermoregulation impairment ............................................................ 12
5.1 Air conditioning compared to other cooling strategies ............................................. 13
6.
Air conditioning and other cooling systems ................................................................. 14
6.1 Cooling garments .................................................................................................... 14
6.2 Fans ......................................................................................................................... 15
6.3 Evaporative cooling ................................................................................................. 15
6.4 Air conditioning (refrigerated cooling) ...................................................................... 15
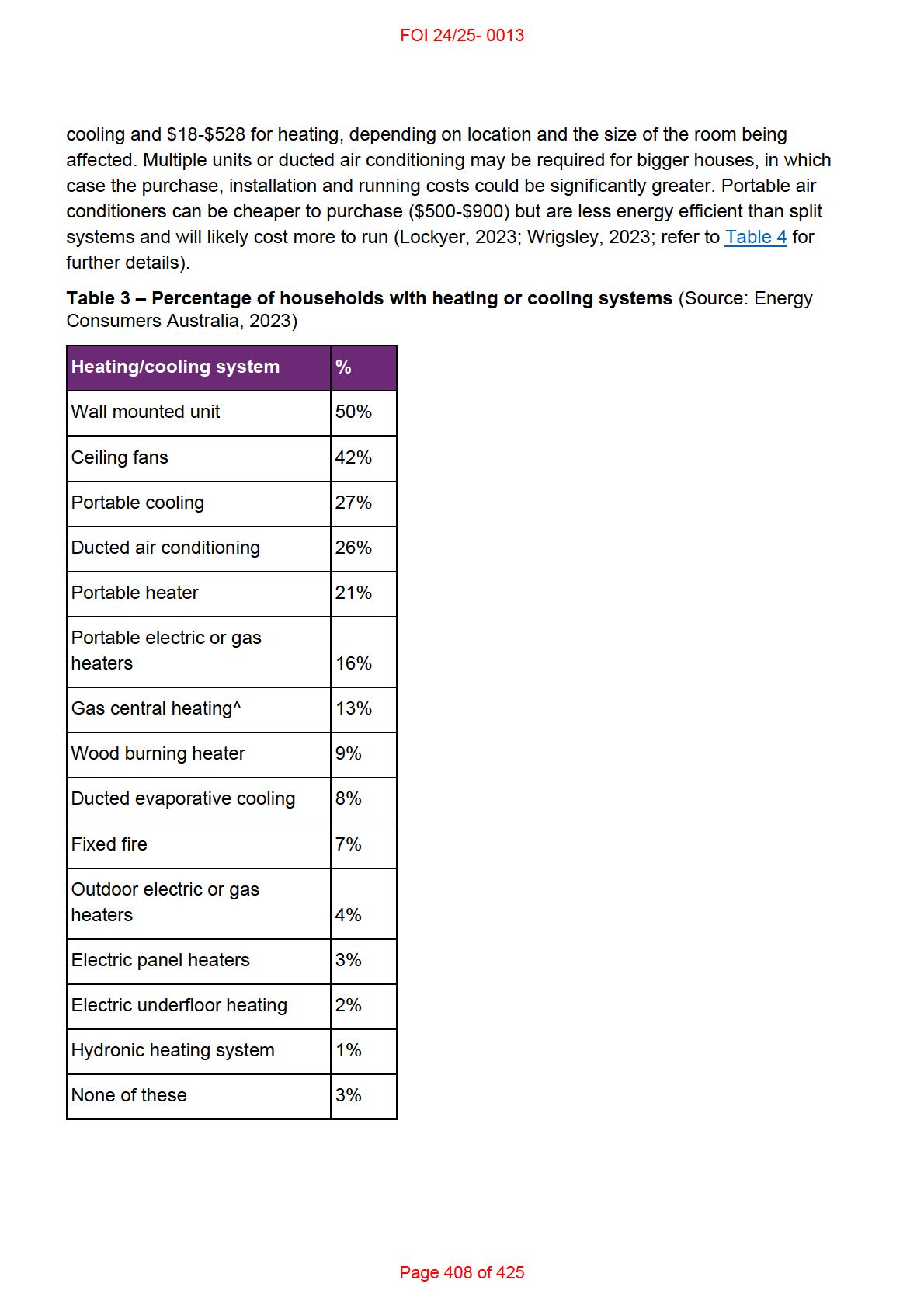
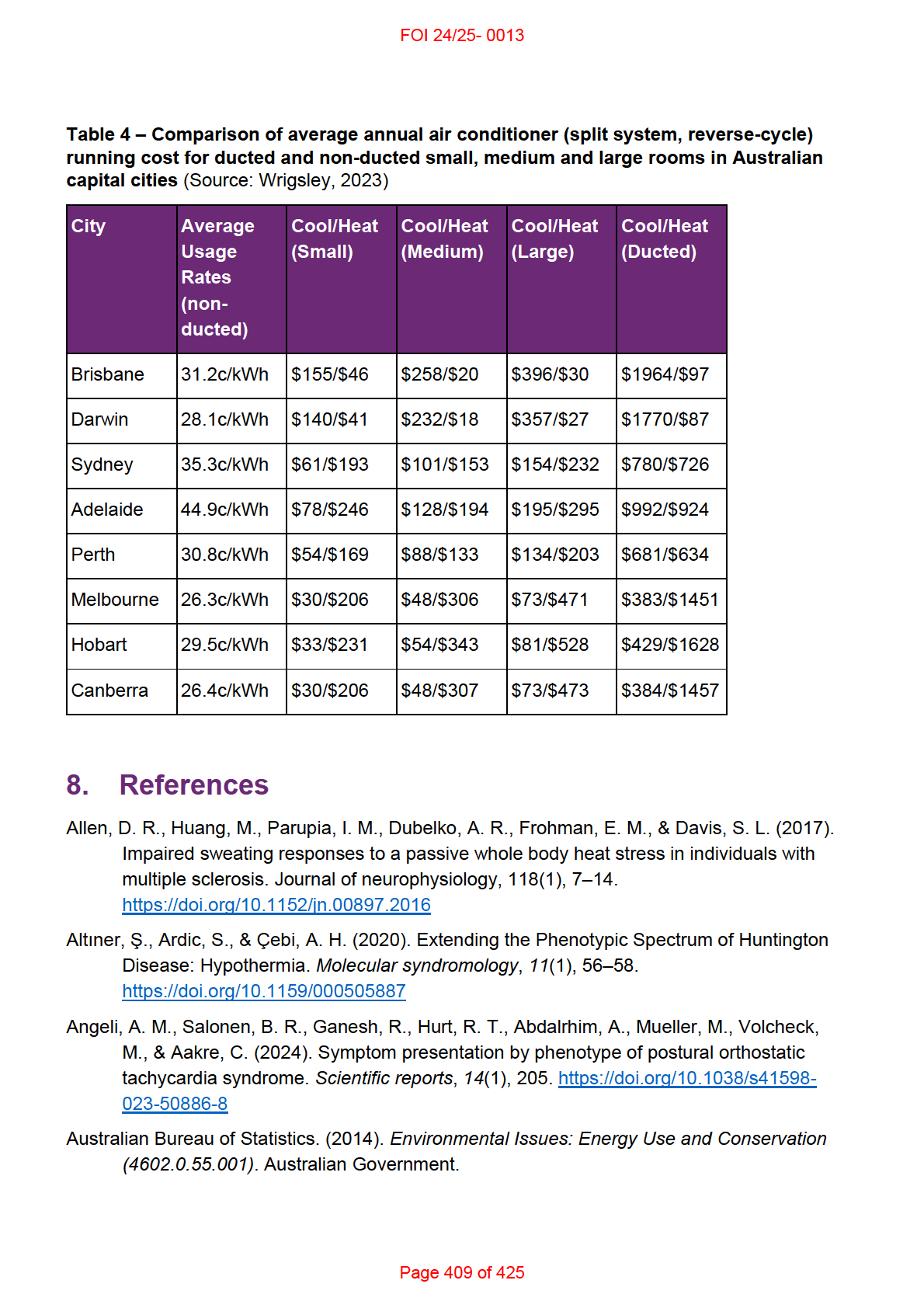
7.
Air conditioning use in Australia .................................................................................. 17
8.
References ................................................................................................................. 19
Page 392 of 425
FOI 24/25- 0013
2. Summary
Note: This paper is a substantial revision of a research paper originally completed in October
2019 and reviewed in February 2024.
Thermoregulation impairment can result from a wide range of health conditions and
disabilities. The human thermoregulatory system involves perceptual, physiological and
behavioural components. A condition may result in a thermoregulatory impairment if it affects
the peripheral or central nervous systems, or if the condition impacts strength, mobility, motor
control, cognition or emotional regulation.
The main types of cooling systems found in Australian homes are fans, evaporative and
refrigerative air conditioners. Refrigerative air conditions, including reverse cycle air
conditioners, are the most common type of air conditioner used in Australia. The cost-
effectiveness of cooling systems depends on several factors including climate, location, energy
prices, architectural features of the home, device running time, temperature set-point and other
lifestyle factors.
There is evidence for the benefits of air conditioner use in the general population to manage
the effects of heat, especially in very hot and dry climates. However, there is very little
evidence comparing air conditioning with other cooling devices or strategies and very little
experimental evidence showing the circumstances in which air conditioning might contribute to
managing the symptoms of thermoregulation impairment.
Despite this, public health messaging and recommendations from researchers and clinicians
are consistent. They suggest that simple behavioural strategies and easily accessible cooling
devices have a role in managing the symptoms of thermoregulation impairment. Behavioural
strategies include:
• understanding personal heat tolerance and preferences
• staying inside during the hotter times of day
• planning outdoor or strenuous activities for cooler times of day
• wearing loose or light clothing
• wearing wet clothes or wraps
• taking regular breaks from activity
• consuming cold foods and drinks
• taking cold baths or showers.
Recommended equipment or devices include:
• space coolers (including evaporative coolers and air conditioning)
• electric fans
• cooling garments.
Page 393 of 425
FOI 24/25- 0013
3. Human thermoregulation
Humans are homeothermic animals, which means that human body temperature is maintained
at a nearly constant level largely, but not entirely, independent of the environment. Core
human body temperature is maintained at around 37°C (+/- 0.5°C), while peripheral body
temperature may vary more widely (Romanovsky, 2018; Cheshire, 2016).
When the core body temperature is too low, this is called hypothermia. When the core body
temperature is too high, this is called hyperthermia. Some sources refer to hypo and
hyperthermia as any variation outside the normal range of core body temperature.
(Romanovsky, 2018). Other sources define states more specifically as below 35°C for
hypothermia and above 40°C for hyperthermia (Cheshire, 2016).
Slight changes outside the accepted range can be controlled with physiological or behavioural
responses. Extreme changes to core body temperature may lead to significant injury or death
(Osila et al, 2023; Cheshire, 2016). Age can affect the ability to regulate body temperature due
to both physiological changes (such as changes in metabolism or the cardiovascular system)
and behavioural changes (spending more time at home, reduced activity), which is why older
people are more susceptible to complications from environmental extremes (Osila et al, 2023;
Bennetts et al, 2020).
Thermoregulation is the process of maintaining body temperature by balancing heat
generation and heat loss. Temperature variations are picked up by thermoreceptors on the
skin or inside the body. These receptors alert the thermoregulatory centre located in the
hypothalamus to enact thermoeffectors, physiological or behavioural responses that regulate
body temperature.
3.1 Thermoeffectors
Physiological thermoeffectors are involuntary body processes that help to control heat loss or
heat generation. They include:
• skin vasodilation or vasoconstriction
• sweating
• shivering
• piloerection
• panting.
Behavioural thermoeffectors are voluntary or instinctual complex behaviours. They include
behaviours such as changing posture, drinking water, adding or removing clothing, turning on
a fan or air conditioning etc (Osila et al, 2023; Romanovsky, 2018).
Thermoeffectors aid in heat loss, conservation or generation by affecting one or more of the
four processes of heat exchange: conduction, convection, radiation, and evaporation (Osila et
al, 2023; Romanovsky, 2018; Cheshire, 2016).
Page 394 of 425
FOI 24/25- 0013
Conduction
Conduction occurs when heat is transferred from one object to another object in direct contact.
Materials with high conductivity are more able to draw heat away from the body. For example,
water has a high conductivity and so submersion in water is a good way to draw heat from the
body (Osila et al, 2023; Romanovsky, 2018).
Convection
Convection occurs when a body is submerged in a gas or liquid. Movement of the fluid
replaces layers of fluid closer to the body with fluid further from the body. The layers of fluid
closer to the body have a temperature closer to the temperature of the skin, while the more
distant fluid has a temperature closer to the ambient temperature. Convection therefore
intensifies conduction. If the environment is hotter, the body is exposed to hotter material and
so heats up faster. If the environment is colder, the body is exposed to colder material and so
cools down faster. For example, a ceiling fan cools by convection by increasing movement of
air on the skin, removing warmer air closer to the body and replacing it with cooler air further
from body (Osila et al, 2023; Romanovsky, 2018).
Radiation
All materials emit and absorb heat via radiation in the form of electromagnetic waves. The
human body loses approximately 60% of its heat via radiation. Unlike conduction or
convection, radiation does not require contact with a medium. For example, solar radiation can
warm the earth despite passing through colder layers of earth’s atmosphere (Osila et al, 2023;
Connor, 2022; Romanovsky, 2018; Cheshire, 2016).
Evaporation
Liquid requires energy in the form of heat to evaporate. The heat required is drawn from the
environment or from the liquid itself and transferred from the liquid to the gas. For example,
animals make use of evaporative cooling in the form of sweating and panting (Osila et al,
2023; Romanovsky, 2018; Lohner, 2017). Evaporation accounts for about 22-30% of heat lost
from the body (Osila et al, 2023; Cheshire, 2016). Evaporation is the most efficient form of
heat loss in the human body, though it can be less effective in more humid environments and
does consume large amounts of water. Evaporation is the only form of heat transfer that also
works when the ambient temperature is higher than the temperature of the skin (Romanovsky,
2018).
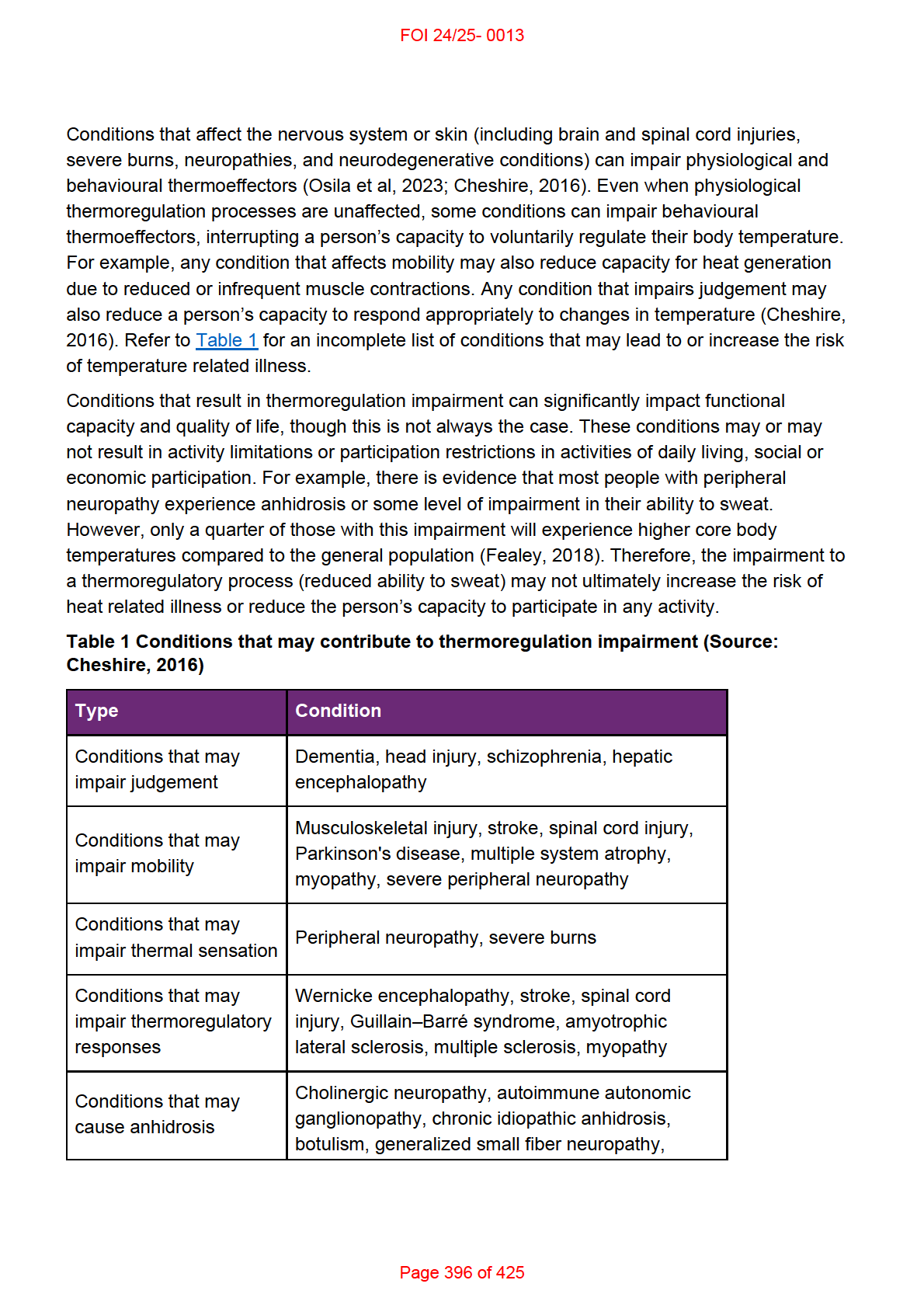
4. Conditions resulting in thermoregulation impairment
Some conditions can impair our thermoregulatory processes and therefore increase the risk of
temperature related health problems. The sections below describe some, though not all,
conditions for which there is evidence of thermoregulatory impairment. For most conditions,
whether thermoregulation impairment occurs, or whether the impairment is substantial and
results in activity limitations or participation restrictions, will vary for individuals.
Page 395 of 425
FOI 24/25- 0013
Sjögren syndrome, multiple system atrophy,
Fabry's disease, bilateral cervical sympathectomy
Conditions that may
Status epilepticus, neuroleptic malignant
increase thermogenesis syndrome, malignant hyperthermia
Other conditions that
Hypoglycemia, Diabetic ketoacidosis,
may lead to
Hypothyroidism, Adrenal failure, Hypopituitarism,
thermoregulatory
Renal failure, Shock, Sepsis, Anorexia nervosa,
impairment
Thyrotoxicosis, Pheochromocytoma
4.1 Spinal cord injury
There is evidence of impaired thermoregulation in people with spinal cord injury, mostly likely
due to a combination of reduced activity of thermoreceptors to detect changes in temperature,
reduced muscle mass and impairment in thermoeffectors such as sweating, vasoconstriction
and vasodilation (Osila et al, 2023; Grossman et al, 2021; Zhang, 2019; Price & Trbovich,
2018; Cheshire, 2016; Girard, 2015). People with higher level of lesion show greater
thermoregulatory impairment (Osila et al, 2023; Grossman et al, 2021). There is evidence that
people with spinal cord injury below the level of T6 can regulate body temperature as
effectively as people without spinal cord injury (Grossman et al, 2021; Price & Trbovich, 2018).
There is some evidence that thermoregulation impairment in people with spinal cord injuries
above T6 may also lead to activity limitations. For example, high or low temperatures may
prevent people with tetraplegia from participating in activities outside the home (Price &
Trbovich, 2018).
4.2 Acquired brain injury
Thermoregulatory impairment after brain injury (traumatic brain injury or stroke) may involve
injury to the hypothalamus, changes in blood flow, vascular control and metabolism, and
difficulties with mobility or judgement (Gowda et al, 2018; Cheshire, 2016; Thompson et al,
2003). There is evidence that around 70% of people experience hyperthermia during the acute
phase after traumatic brain injury. This may be due to the nature of the injury, post-traumatic
inflammation or post-injury infection (Thompson et al, 2003). Hyperthermia is a risk factor for
secondary injury. This includes rebound hyperthermia, which is a possible consequence of
rewarming after induced hypothermia (Gowda et al, 2018; Childs & Lunn, 2013). Clinicians
regularly induce hypothermia soon after the initial brain injury to prevent secondary brain injury
and improve other outcomes. Thermoregulatory impairment may be more common in some
people with brain injury, though affected sub-groups have not been identified (Gowda et al,
2018).
Page 397 of 425
FOI 24/25- 0013
4.3 Parkinson’s Disease
Thermoregulation difficulties are common in people with Parkinson’s disease and may lead to
difficulties with sweating, sleep, and altered perception of heat and cold (Pfeiffer, 2020; Coon
& Low, 2018; Zhong et al, 2013). The presence of peripheral neuropathy in people with
Parkinson’s disease can result in impairments to thermoeffectors such as
vasoconstriction/dilation, sweating and piloerection (Coon & Low, 2018). Around 30-70% of
people with Parkinson’s experience problems with sweating, including hyperhidrosis
(increased sweating) and hypohidrosis (reduced sweating). This may be related to
neurological changes or to medications used to treat the core symptoms of Parkinson’s
disease. Hypohidrosis can increase risk of overheating, while hyperhidrosis can be
uncomfortable and lead to sleep difficulties (Pfeiffer, 2020; Jost, 2017). Thermoregulation
impairment can affect well-being and quality of life for people with Parkinson’s disease:
Patients are often bothered by heat intolerance which may influence activity levels and
social endeavors. Needing to frequently change clothing or bedding due to excessive
sweating episodes is also problematic for patients and their caregivers, particularly
when motor function is compromised. Temperature intolerance or night sweats may
impair a patient’s sleep, which is often affected due to motor dysfunction or concomitant
sleep disorders. Social function is also affected by sweating episodes, leaving some
patients to feel embarrassed and contributing to social isolation (Coon & Law, 2018,
p.271).
4.4 Multiple Sclerosis
Thermoregulation impairment is more researched in multiple sclerosis than for any other
condition. Around 60-80% of people with multiple sclerosis experience temperature sensitivity.
Thermoregulatory dif iculties in people with multiple sclerosis, especially susceptibility to
hyperthermia, may be due to impaired sweating function, decreased sensitivity of
thermoreceptors or hypothalamic dysfunction. Hyperthermia is a significant risk as it can
exacerbate symptoms including muscle weakness, spasticity, fatigue, blurred vision and pain,
as well as worsening existing difficulties with balance, processing speed, concentration, and
attention (Osila et al, 2023; Christogianni et al, 2022; Razi et al, 2022; Davis et al, 2018;
Christogianni et al, 2018; Al en et al, 2017). Hyperthermia may be induced by environmental
increases in temperature, hot baths or exercise (Razi et al, 2022; Christogianni et al, 2022;
Davis et al, 2018; Christogianni et al, 2018). However, there is evidence that regular exercise
for people with multiple sclerosis can improve symptoms and quality of life. Therefore, heat
management strategies should be in place when clinicians recommend an exercise program
for people with multiple sclerosis (Huang et al, 2015). Cold temperatures can also lead to a
worsening of symptoms, though this is less common and less studied (Christogianni et al,
2018).
Page 398 of 425
FOI 24/25- 0013
4.5 Peripheral neuropathy
Peripheral neuropathy is a general term for conditions that cause damage to the nerves of the
peripheral nervous system. Damage can occur to large-diametre or small-diametre nerve
fibres. Large fibres mediate motor and sensory functions, while small fibres mediate autonomic
functions, pain and temperature (Novello & Pobre, 2023; Castelli et al, 2020).
Conditions that can result in peripheral neuropathy include Guil aine-Barre syndrome, diabetes
mellitus, Fabry disease, Parkinson’s disease, Ehlers Danlos syndrome, postural orthostatic
tachycardia syndrome (POTS) and Sjögren syndrome. Diabetes related peripheral neuropathy
is the most prevalent form of the peripheral neuropathy in developed countries (Osila et al,
2023; Fealey, 2018; Cheshire, 2016).
There is evidence that most people with some form of peripheral neuropathy experience
abnormalities in core body temperature. Common thermoregulatory concerns for people with
peripheral neuropathy include impairments to physiological thermoeffectors such as
vasoconstriction/dilation, sweating, piloerection and shivering (Fealey, 2018; Cheshire, 2016).
As peripheral neuropathy is associated with reduced sensitivity of thermoreceptors, there is
also reason to believe the condition may lead to disruption of behavioural thermoeffectors
(Fealey, 2018).
Heat intolerance is a possible symptom of POTS. High ambient temperatures may also
exacerbate core symptom of orthostatic intolerance. (Fedorowski, 2018; Landero, 2014;
Goodkin & Bellew, 2014). These symptoms may be associated with the presence of small fibre
neuropathy. In a study of 276 participants with POTS, Angeli et al (2024) found 35% showed
altered sweat patterns, which characterised the neuropathic phenotype. A small study of 30
people with POTS found significant differences in thermal perception and pain threshold (Bil ig
et al, 2020). POTS is also a common co-occurring condition in Ehlers Danlos syndrome, which
itself can present with thermoregulatory dif iculties (Colman et al, 2023; Thwaites et al, 2022;
Hakim et al, 2017).
4.6 Psychosocial conditions
While there is preliminary evidence that some people with anxiety disorders show
abnormalities in physiological thermoeffectors such as vasodilation and sweating (Fischer et
al, 2021), psychosocial conditions may coincide with thermoregulatory impairments in the form
of altered sensation or disrupted behavioural thermoeffectors (due to altered cognition,
judgement or executive control). RES 319 Weather and Bipolar Disorder contains some
discussion of the effects of temperature on outcomes for people with bipolar and other
psychosocial conditions.
Page 399 of 425
FOI 24/25- 0013
4.7 Epilepsy and seizure disorders
Temperature may affect epilepsy and seizure activity differently, depending on the individual,
the type of epilepsy or type of seizure.
Hyperthermia is both a possible trigger and a possible consequence of seizure. It may be a
consequence of seizure due to excessive muscle activity or activation of the autonomic system
(Pollandt & Bleck, 2018; Cheshire, 2016). Hyperthermia can also cause seizures, as in the
case of febrile seizures experienced mainly by children during episodes of fever. In Dravet
syndrome, seizures can follow even small temperature increases caused by higher ambient
temperatures, fever, cold-warm shifts, warm baths or exercise (Gulcebi et al, 2021; Pollandt &
Bleck, 2018).
However, colder temperatures may also increase risk of seizure in epilepsy. Hospital
admission studies in Taiwan, Germany and Korea found that seizure risk increases in colder
temperatures (Chang et al, 2019; Kim et al, 2017; Rakers et al, 2017). However, these studies
take place in climates that tend to have mild summers and may not generalise to Australia. For
example, Rakers et al (2017) found that ambient temperatures higher than 20°C decrease the
risk of seizure, though the highest recorded temperature in the study was 28°C.
Epilepsy Action Australia (n.d.) states:
Whilst research related to weather and seizures has been limited, and based in the
northern hemisphere, there is no scientific evidence that hot weather itself causes
seizures to occur in people with epilepsy. In Australia it appears most people report that
the heat, or becoming overheated, tends to increase the likelihood of seizures.
Becoming severely overheated can cause seizures, but an average hot day is not in
itself the culprit.
Obviously, heat can be a major contributor to dehydration. If someone is exposed to
heat for a long period of time and does not drink enough fluid, this can cause
dehydration which can increase the risk of a seizure in someone with epilepsy,
sometimes later in the day. When fluid loss from the body (mostly perspiration) is
greater than fluid intake, it causes a change in electrolytes – a drop in sodium (salt) and
glucose (sugar) levels in the body. Ultimately, this can lead to low blood sugar levels
(hypoglycemia) which can also trigger seizures for some people.
4.8 Autism
People with autism may experience sensory differences such as hypo or hypersensitivity to
heat or cold (Raising Children Network, 2024; Zaniboni et al, 2023; Hidaka et al, 2023). Based
on their review, Zaniboni et al suggest the following sensory dif erences with respect to
perception of heat and cold:
Page 400 of 425
FOI 24/25- 0013
• Different tactile sensitivity, as well as higher variability in warm and cold detection:
paradoxical heat sensation (the perception of heat when it should not be perceived,
hyper-sensitivity), lower thresholds in heat and cold detection (hypo-sensitivity).
• Thermal processing might be related with environment adoption or self-injury.
• Difficulties with interoception (heart-rate and body-temperature perception) and self-
regulation and identification of emotions.
• Differences in hypothalamus development (related to homeostasic regulation, including
metabolic rate, temperature and emotion). This can also lead to depression, anxiety,
sleep disorders and obesity (2023, p.10).
4.9 Motor neurone disease / Amyotrophic lateral sclerosis
There is a lack of evidence regarding thermoregulatory impairments in motor neurone
diseases such as amyotrophic lateral sclerosis (ALS). It is likely that behavioural
thermoeffectors are impaired in ALS considering symptoms related to mobility and cognitive
functions. There is minimal evidence that people with ALS experience altered heat sensation
and that hypothalamus volume may be reduced. Physiological thermoeffectors such as
shivering may be affected by progressive impairment in skeletal muscles (Dupuis et al, 2018).
Much of the evidence for involvement of thermoregulatory systems in ALS comes from studies
of animal models (Rodríguez-Sánchez et al, 2022; Braun et al, 2019). In their review of the
subject, Dupuis et al state:
In our clinical experience, we observed that ALS patients often complain of feeling hot,
or conversely of being unable to warm up, and some patients develop low body
temperature. Also, some patients report a worsening of symptoms in cold weather.
However, these symptoms are generally not considered as being part of the core clinical
picture, mostly because they are attributed to muscle atrophy and/or nerve
degeneration. Therefore, potential thermoregulatory defects to the best of our
knowledge have never been systematically studied in ALS patients (2018, p.750).
Since then, at least one study has shown a high rate of hypothermia in people with ALS who
have had tracheostomy or invasive ventilation for longer than five years (Nakayama et al,
2018).
4.10 Huntington’s disease
Thermoregulation problems are sometimes reported by people with Huntington’s disease:
some clinicians do occasionally report anecdotally that some of their [Huntington’s
disease] patients seem to have a striking indifference to cold and that they wil dress too
lightly for the weather, while others wil sweat so profusely that they resort to wearing
cooling vests (Weydt et al, 2018, p.766).
The first case study of a person with Huntington’s disease presenting with hypothermia was
submit ed in 2020 (Altiner et al, 2020). Most of the evidence of thermoregulation impairment in
Page 401 of 425
FOI 24/25- 0013
Huntington’s disease comes from animal models. These studies have shown evidence of
hypothermia, weight loss, involuntary movements, as well as differences in circadian rhythms,
brown adipose tissue, skeletal muscle and the hypothalamus. This suggests a possible effect
of Huntington’s disease on heat retention, shivering and non-shivering thermogenesis.
Development of psychiatric conditions and problems with mobility and cognitive function may
also contribute to disruption of behavioural thermoeffectors. There are few studies directly
investigating thermoregulation associated with Huntington’s disease in humans (Altiner et al,
2020; Weydt et al, 2018).
4.11 Severe burns
The skin plays an important role in thermoregulatory processes including heat retention,
sensation, sweating, piloerection, vasodilation and vasoconstriction. When large parts of the
skin are lost or damaged, this enables increased heat loss and contributes to difficulties
sensing changes in temperature, thereby increasing the risk of hypothermia. People with
severe burns are also at risk of hypermetabolism, which can lead to hyperthermia, excessive
sweating, weight loss, muscle wasting and other symptoms (Radzikowska-Büchner et al,
2023; Mertin et al, 2022). In cases of severe burn injury, metabolic changes can last up to
three years after the initial injury and function of damaged skin may not return (Radzikowska-
Büchner et al, 2023; Jeshke et al, 2011).
5. Management of thermoregulation impairment
Researchers and clinicians have recommended behavioural strategies to manage
thermoregulation impairment in people with multiple sclerosis (Christogianni et al, 2022; Davis
et al, 2018), autism (Zaniboni et al, 2023), and spinal cord injury (Girard, 2015). Behavioural
strategies can include moving to a cooler area, planning activities for cooler times of the day,
taking regular breaks from strenuous activity, choosing weather appropriate clothing, or
gradual acclimatisation in warmer or colder temperatures (Healthdirect, 2024; Zaniboni et al,
2023; Grossman et al, 2021; Davis et al, 2018; Girard, 2015; Australian Red Cross, n.d.).
Standard first line treatment for hyperthermia includes cooling strategies that are usually low
cost or readily accessible: air conditioning, misting fans, cold bath or shower, drinking cold
water and applying cold packs or ice packs (Healthdirect, 2024; Grossman et al, 2021;
Christogianni et al, 2022; Davis et al, 2018; Gowda et al, 2018; Hopkins et al, 2018;
Zawardska et al, 2017; Cheshire, 2016; Australian Red Cross, n.d.). These non-invasive
methods are less easy to control than invasive cooling strategies such as intravenous injection
of cooling substances. Where non-invasive strategies succeed in lowering body temperature,
they are not easily able to maintain a stable target temperature and therefore require
monitoring and adjustment (Gowda et al, 2018).
There is evidence of effectiveness of non-invasive cooling strategies to improve exercise
performance and lower the risk of heat related effects of exercise in the general population
(Heydenreich et al, 2023; Douzi et al, 2019). There is mixed evidence for the effectiveness of
Page 402 of 425
FOI 24/25- 0013
non-invasive strategies in people with thermoregulatory impairment. The inconsistency in the
evidence may be due to the frequency of smal , low powered studies and the heterogeneity of
climatic conditions and outcome measures (Grossman et al, 2021).
In a review of cooling strategies for people with spinal cord injury, Grossman et al (2021) found
inconsistent evidence for the temperature reducing effects of cooling garments, cold drinks
and misting fans. Some studies show cooling garments reduce skin temperature but not core
body temperature, whereas a consistent effect across several studies showed pre-cooling
using cooling garments or other methods could improve endurance during exercise and lower
rate of increase of body temperature (Grossman et al, 2021; Davis et al, 2018).
A 2023 systematic review into the use of cooling garments for people with Multiple Sclerosis
found that cooling garments are effective in reducing body temperature and improving walking
capacity and functional mobility (Stevens et al, 2023). The authors found no significant
differences between types of cooling garment. Active treatment groups were compared with
either other cooling garments, sham active controls or passive controls. No study was
reviewed that compared cooling garments with other cooling strategies such as air
conditioning.
5.1 Air conditioning compared to other cooling strategies
Researchers and clinicians have recommended reducing the ambient temperature of the
environment with space cooling strategies/devices as a way of managing thermoregulation
impairment in people with multiple sclerosis (Christogianni et al, 2022; Davis et al, 2018),
autism (Zaniboni et al, 2023), spinal cord injury (Price & Trbovich, 2018), epilepsy (Epilepsy
Action Australia, n.d.), and severe burns (Radzikowska-Büchner et al, 2023).
Existing evidence indicates that air conditioning has a role in managing thermoregulation
impairment. Hospital studies show air conditioning can improve or maintain patients’ thermal
comfort, recovery rates and well-being, and reduce infections and length of hospital stays.
However, more research is required to determine the optimum ambient temperature to
maximise patient outcomes (Lenzer et al, 2020; Shajahan et al, 2019). In the case of severe
burns, raising the ambient temperature of the room to 24°C – 38°C may prevent or reduce the
risk of a hypermetabolic reaction (Radzikowska-Büchner et al, 2023).
There are very few studies in which air conditioning is assessed as an intervention aimed to
manage thermoregulation impairment. In a survey study of 438 heat-sensitive people with
multiple sclerosis, Christogianni et al (2022) found that around three quarters used air
conditioning to manage risks of overheating. However, in a review of cooling
therapies/interventions for people with multiple sclerosis, Bilgin et al (2022) did not find any
studies that used any conditioning as an intervention.
No studies were found comparing the use of air conditioning with other cooling methods in
il ness management or treatment. One study compared the use of air conditioning with electric
fans in the general population (Morris et al, 2021). The authors found that electric fans are an
Page 403 of 425
FOI 24/25- 0013
appropriate way to manage risk of heat stress for adults in Australia when the ambient
temperature is under 38°C. However, the authors also examined older people taking
medication that may impair sweating function. They found impaired sweating function lowers
the effectiveness of electric fans. This is because fans cool by both convection and
evaporation (refer to 6.2 Fans for more detail). Therefore, the authors recommend
supplementing electric fan use with air conditioning systems for people with impaired sweating
function.
Most recommendations cited above are based on clinical opinion. Furthermore, the
recommendations focus on achieving or maintaining cool indoor air temperatures, and rarely
mention the means to achieve those temperatures. They do not differentiate between air
conditioning and other space cooling strategies (evaporative cooling, ceiling fans, passive
cooling).
6. Air conditioning and other cooling systems
Common home cooling systems include fans, evaporative cooling or refrigerated cooling.
Sometimes the term air conditioning is used to refer to all these systems. Most often it is used
to refer only to refrigerated cooling systems.
Not all systems wil be appropriate in all circumstances. The most appropriate air conditioning
system for a person wil depend on factors including:
• environment – regional climate, average temperature, humidity
• building – size, layout, solar power, air flow and other passive cooling features
• occupancy – whole house or single room, rent or own, number of residents
• lifestyle – budget, habits, cooling needs, sustainability preferences (Wrigsley, 2023;
Barnes, 2023; Lockyer, 2023; Milne et al, 2020; Gilmour & Steen, n.d.).
6.1 Cooling garments
Cooling garments can include jackets, vests, hats, hoods, gloves, wrist bands and thigh straps
(Stevens et al. 2023; Laique & Hussain, 2018). Ren et al (2022) identify six types of cooling
mechanism used in garments:
• ice cooling – garment contains insulated pockets to hold ice
• phase change materials cooling – made from a designed material that uses the latent
heat from the body to lower the temperature of the microclimate between the body and
the garment
• radiative cooling – made from a designed material that aims to maximise heat loss
allowing more infrared radiation to escape the body
• thermo-electric cooling – garment contains conductors which can be used to directly
draw heat energy from the body as an electric current is passed through the conductor
• liquid cooling – garment contains pipes carrying cold liquid and a pump to ensure liquid
is spread over the garment
Page 404 of 425
FOI 24/25- 0013
• air-cooling – garment that maximises ventilation through the use of design and small
electric fans.
6.2 Fans
Fans work by moving air around a room more quickly. They do not cool the air, but rather aid
the body’s thermoregulatory processes. Faster moving air helps sweat evaporate more quickly
(evaporation) and blows cooler air at the skin (convection). Fans are less effective in higher
temperatures, though the exact threshold is stil being debated in the literature (Morris et al,
2021; Milne et al, 2020; Iorio, 2019). Fans can be effective for healthy adults in temperatures
up to 38°C (Morris et al, 2021) and may help to a lesser extent up to 42°C (Iorio, 2019). The
Australian government’s Your Home site states:
Fans should be the first appliance of choice for cooling. They are cheap to run and
generally use less energy than evaporative coolers or air-conditioners. Typically, the air
flow created by a fan provides a similar improvement to comfort as reducing the
temperature by around 3°C. With good design and insulation, fans can often supply
adequate cooling for acclimatised residents in all Australian climates (Department of
Climate Change, Energy, the Environment and Water; n.d).
Fans are most effective when aimed directly toward the body, in humid climates or when used
in combination with water spray, wet clothing or wraps (Morris et al, 2021; Milne et al, 2020;
Iorio, 2019; Department of Climate Change, Energy, the Environment and Water; n.d.).
6.3 Evaporative cooling
An evaporative cooler blows cool, humid air into a space by drawing outside air through a wet
filter which is then expelled by a fan. An evaporative cooler may be less expensive to purchase
and run than an air conditioning system, but this depends on the model. Evaporative coolers
are less effective in humid environments and require large amount of water to operate (Milne
et al, 2020; Department of Climate Change, Energy, the Environment and Water; n.d.).
6.4 Air conditioning (refrigerated cooling)
An air conditioning system that operates by refrigerated cooling draws warm air from inside the
space and cools it via contact with a refrigerant gas. The cool air is blown back into the space
and the extracted heat is expelled outside (Barnes, 2023; Milne et al, 2020; Barnes, 2019;
Department of Climate Change, Energy, the Environment and Water; n.d.). Air conditioning
systems can vary by cost, size, energy efficiency and type of refrigerant used. Air conditioners
can be:
• fixed or portable
• single unit, split system, or multi-split system
• ducted or non-ducted
Page 405 of 425
FOI 24/25- 0013
• reverse cycle or cooling only (Wrigsley, 2023; Barnes, 2023; Department of Climate
Change, Energy, the Environment and Water, n.d.; Milne et al, 2020).
For comparison of purchase and running costs of different air conditioning systems in
Australia, refer to 7. Air conditioning in Australia.
Reverse cycle air conditioning
A reverse cycle air conditioner operates in a similar way to a cooling-only system. However, a
reverse cycle system is also able to reverse the refrigeration process, sending cold air outside
and warm air inside. Reverse cycle air conditioners are often considered the most efficient
systems because they can provide both heating and cooling. However, energy efficiency
ultimately depends on a range of factors (Department of Climate Change, Energy, the
Environment and Water, n.d.; Milne et al, 2020; Barnes, 2019).
Single unit, split system, or multi-split system air conditioning
Split system air conditioners have an outside unit and an inside unit. They are the most
common fixed air conditioning systems and are usually more energy efficient than single unit
systems. Split systems can be ducted or non-ducted. Multi-split systems have an outside unit
and multiple indoor units, which can be placed in dif erent rooms. They are an alternative to
ducted systems (Barnes, 2023; Department of Climate Change, Energy, the Environment and
Water, n.d.; Milne et al, 2020; Barnes, 2019).
Single unit systems are generally suited to smaller areas. They are generally less energy
efficient than split systems. They can be fixed or portable. Portable systems are generally less
expensive to purchase than fixed systems. They may be appropriate for smaller areas or when
the system needs to be moved to different areas. They may also be appropriate when
installing a fixed unit is not feasible, such as in rental properties (Lockyer, 2023; Milne et al,
2020; Barnes, 2019).
Ducted air conditioning
A ducted system is a central heating or cooling system, which means it is designed to warm or
cool a whole house or building rather than a single room. Ducted systems can be evaporative
coolers, reverse-cycle split systems or cooling only split systems. There is usually an outdoor
unit on the roof and an indoor unit under the floor or in the ceiling. Ducts extend from the
indoor unit and into multiple rooms or multiple areas of a bigger space (Department of Climate
Change, Energy, the Environment and Water, n.d.; Milne et al, 2020; Barnes, 2019).
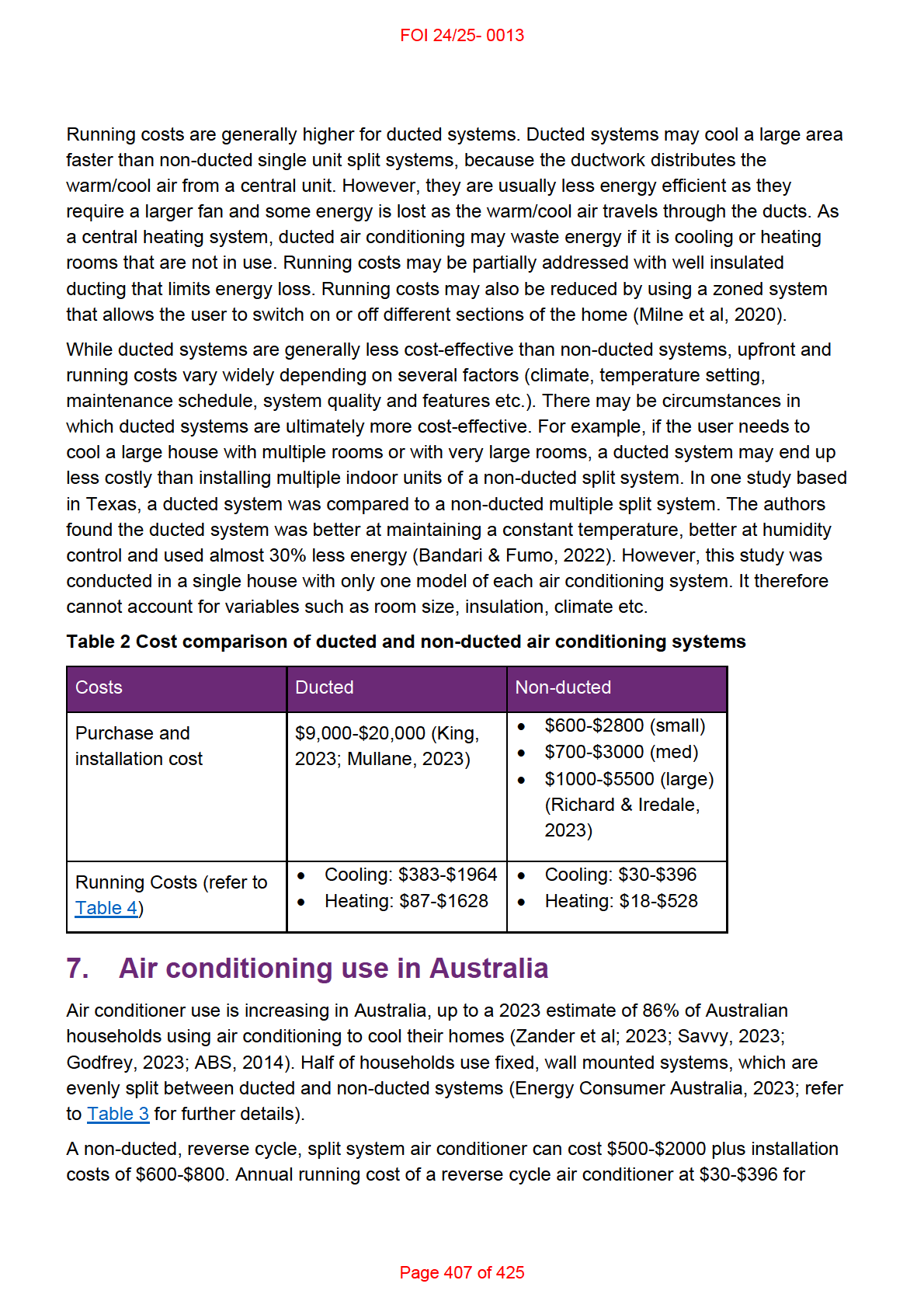
In terms of cost, ducted systems are generally more expensive to purchase, install and run,
and therefore are generally less cost effective than non-ducted systems (refer to Table 2).
Installation is a significant upfront cost for ducted systems as work is required to install the roof
unit as well as ducts throughout the home. Furthermore, ducted systems are not possible in
some houses due to lack of space or other architectural features (King, 2023; Mullane, 2023).
Page 406 of 425
FOI 24/25- 0013
https://www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/4602.0.55.001Mar%202014
?OpenDocument
Australian Red Cross. (n.d.).
Heatstroke and heat exhaustion.
https://www.redcross.org.au/emergencies/prepare/heatstroke-and-heat-exhaustion/
Barnes, C. (2023).
What to know before buying an air conditioner. CHOICE.
https://www.choice.com.au/home-and-living/cooling/air-conditioners/buying-guides/air-
conditioners
Barnes, C. (2019).
How to buy ducted reverse-cycle air conditioning. CHOICE.
https://www.choice.com.au/home-and-living/cooling/ducted-reverse-cycle-air-
conditioning/buying-guides/ducted-reverse-cycle-air-conditioning
Bennetts, H., Arakawa Martins, L., van Hoof, J., & Soebarto, V. (2020). Thermal Personalities
of Older People in South Australia: A Personas-Based Approach to Develop Thermal
Comfort Guidelines. International journal of environmental research and public health,
17(22), 8402. https://doi.org/10.3390/ijerph17228402
Bhandari, M. & Fumo, N. (2022). Comparison Study of a Traditional Ducted Heat Pump and a
Multi Split Heat Pump.
International Refrigeration and Air Conditioning Conference.
Paper 2321. https://docs.lib.purdue.edu/iracc/2321
Bil ig, S. C. I., Schauermann, J. C., Rolke, R., Katona, I., Schulz, J. B., & Maier, A. (2020).
Quantitative sensory testing predicts histological small fiber neuropathy in postural
tachycardia syndrome.
Neurology, Clinical practice,
10(5), 428–434.
https://doi.org/10.1212/CPJ.0000000000000770
Braun, M. C., Castillo-Ruiz, A., Indic, P., Jung, D. Y., Kim, J. K., Brown, R. H., Jr, Swoap, S. J.,
& Schwartz, W. J. (2019). Defective daily temperature regulation in a mouse model of
amyotrophic lateral sclerosis.
Experimental neurology, 311, 305–312.
https://doi.org/10.1016/j.expneurol.2018.07.008
Castelli, G., Desai, K. M., & Cantone, R. E. (2020). Peripheral Neuropathy: Evaluation and
Differential Diagnosis.
American family physician, 102(12), 732–739.
Chang, K. C., Wu, T. H., Fann, J. C. Y., Chen, S. L. S., Yen, A. M. F., Chiu, S. Y. H., ... & Liou,
H. H. (2019). Low ambient temperature as the only meteorological risk factor of seizure
occurrence: A multivariate study.
Epilepsy & Behavior, 100, 106283.
Cheshire W. P., Jr (2016). Thermoregulatory disorders and il ness related to heat and cold
stress.
Autonomic neuroscience: basic & clinical, 196, 91–104.
https://doi.org/10.1016/j.autneu.2016.01.001
Childs, C., & Lunn, K. W. (2013). Clinical review: brain-body temperature differences in adults
with severe traumatic brain injury.
Critical Care, 17, 1-17.
Christogianni, A., O'Garro, J., Bibb, R., Filtness, A., & Filingeri, D. (2022). Heat and cold
sensitivity in multiple sclerosis: A patient-centred perspective on triggers, symptoms,
Page 410 of 425
FOI 24/25- 0013
and thermal resilience practices.
Multiple sclerosis and related disorders, 67, 104075.
https://doi.org/10.1016/j.msard.2022.104075
Christogianni, A., Bibb, R., Davis, S. L., Jay, O., Barnett, M., Evangelou, N., & Filingeri, D.
(2018). Temperature sensitivity in multiple sclerosis: An overview of its impact on
sensory and cognitive symptoms. Temperature (Austin, Tex.), 5(3), 208–223.
https://doi.org/10.1080/23328940.2018.1475831
Colman, M., Syx, D., De Wandele, I., Rombaut, L., Wil e, D., Malfait, Z., ... & Malfait, F. (2023).
Sensory profiling in classical Ehlers-Danlos syndrome: a case-control study revealing
pain characteristics, somatosensory changes, and impaired pain modulation. The
Journal of Pain, 24(11), 2063-2078 https://doi.org/10.1016/j.jpain.2023.06.015
Connor, N. (2022).
What is Radiation Heat Transfer – Definition. thermal-engineering.org.
https://www.thermal-engineering.org/what-is-radiation-heat-transfer-definition/
Coon, E. A., & Low, P. A. (2018). Thermoregulation in Parkinson disease.
Handbook of clinical
neurology, 157, 715–725. https://doi.org/10.1016/B978-0-444-64074-1.00043-4
Davis, S. L., Jay, O., & Wilson, T. E. (2018). Thermoregulatory dysfunction in multiple
sclerosis. Handbook of clinical neurology, 157, 701–714. https://doi.org/10.1016/B978-
0-444-64074-1.00042-2
Department of Climate Change, Energy, the Environment and Water. (n.d.).
Heating and
cooling. Australian Government. https://www.energy.gov.au/households/heating-and-
cooling
Douzi, W., Dugué, B., Vinches, L., Al Sayed, C., Hallé, S., Bosquet, L., & Dupuy, O. (2019).
Cooling during exercise enhances performances, but the cooled body areas matter: A
systematic review with meta-analyses.
Scandinavian journal of medicine & science in
sports,
29(11), 1660–1676. https://doi.org/10.1111/sms.13521
Dupuis, L., Petersen, Å., & Weydt, P. (2018). Thermoregulation in amyotrophic lateral
sclerosis.
Handbook of clinical neurology, 157, 749–760. https://doi.org/10.1016/B978-
0-444-64074-1.00046-X
Energy Consumers Australia. (2023).
Energy Consumer Behaviour Survey.
https://ecss.energyconsumersaustralia.com.au/wp-content/uploads/2023/10/ECBS-
October-2023-Household-Toplines.pdf
Epilepsy Action Australia. (n.d.).
E-360 Edition 20: Weather conditions & epilepsy.
https://www.epilepsy.org.au/e-360-edition-20-weather-conditions-epilepsy/
Fealey R. D. (2018). Thermoregulation in neuropathies.
Handbook of clinical neurology, 157,
777–787. https://doi.org/10.1016/B978-0-444-64074-1.00048-3
Fischer, S., Haas, F., & Strahler, J. (2021). A Systematic Review of Thermosensation and
Thermoregulation in Anxiety Disorders.
Frontiers in physiology, 12, 784943.
https://doi.org/10.3389/fphys.2021.784943
Page 411 of 425
FOI 24/25- 0013
Gilmour, K., & Steen, M. (n.d.).
Portable air conditioner buying guide. CHOICE.
https://www.choice.com.au/home-and-living/cooling/portable-air-conditioners/buying-
guides/portable-air-conditioners
Girard O. (2015). Thermoregulation in wheelchair tennis-How to manage heat stress?.
Frontiers in physiology, 6, 175. https:/ doi.org/10.3389/fphys.2015.00175
Godfrey, J. (2023).
Air conditioning usage statistics 2023-2024. Finder.
https://www.finder.com.au/energy/aircon-statistics
Goodkin, M. B., & Bellew, L. J. (2014). Osteopathic manipulative treatment for postural
orthostatic tachycardia syndrome.
The Journal of the American Osteopathic
Association,
114(11), 874–877. https:/ doi.org/10.7556/jaoa.2014.173
Gowda, R., Jaffa, M., & Badjatia, N. (2018). Thermoregulation in brain injury.
Handbook of
clinical neurology, 157, 789–797. https://doi.org/10.1016/B978-0-444-64074-1.00049-5
Grossmann, F., Flueck, J. L., Perret, C., Meeusen, R., & Roelands, B. (2021). The
Thermoregulatory and Thermal Responses of Individuals With a Spinal Cord Injury
During Exercise, Acclimation and by Using Cooling Strategies-A Systematic Review.
Frontiers in physiology, 12, 636997. https://doi.org/10.3389/fphys.2021.636997
Gulcebi, M. I., Bartolini, E., Lee, O., Lisgaras, C. P., Onat, F., Mifsud, J., Striano, P., Vezzani,
A., Hildebrand, M. S., Jimenez-Jimenez, D., Junck, L., Lewis-Smith, D., Scheffer, I. E.,
Thijs, R. D., Zuberi, S. M., Blenkinsop, S., Fowler, H. J., Foley, A., Epilepsy Climate
Change Consortium, & Sisodiya, S. M. (2021). Climate change and epilepsy: Insights
from clinical and basic science studies.
Epilepsy & behavior, 116, 107791.
https://doi.org/10.1016/j.yebeh.2021.107791
Hakim, A., O'Cal aghan, C., De Wandele, I., Stiles, L., Pocinki, A., & Rowe, P. (2017).
Cardiovascular autonomic dysfunction in Ehlers–Danlos syndrome—hypermobile type.
American Journal of Medical Genetics Part C: Seminars in Medical Genetics,
175(1)
168-174 https://doi.org/10.1002/ajmg.c.31543
Healthdirect. (2024).
How to take care of yourself in a heatwave. Australian Government.
https://www.healthdirect.gov.au/blog/how-to-handle-the-heatwave
Heydenreich, J., Koehler, K., Braun, H., Grosshauser, M., Heseker, H., Koenig, D., Lampen,
A., Mosler, S., Niess, A., Schek, A., & Carlsohn, A. (2023). Effects of internal cooling on
physical performance, physiological and perceptional parameters when exercising in
the heat: A systematic review with meta-analyses.
Frontiers in physiology, 14, 1125969.
https://doi.org/10.3389/fphys.2023.1125969
Hidaka, S., Gotoh, M., Yamamoto, S., & Wada, M. (2023). Exploring relationships between
autistic traits and body temperature, circadian rhythms, and age.
Scientific reports,
13(1), 5888. https://doi.org/10.1038/s41598-023-32449-z
Page 412 of 425
FOI 24/25- 0013
Hopkins, P., Gupta, P. K., & Bilmen, J. G. (2018).
Malignant hyperthermia.
Handbook of
clinical neurology, 157, 645–661. https://doi.org/10.1016/B978-0-444-64074-1.00038-0
Huang, M., Jay, O., & Davis, S. L. (2015). Autonomic dysfunction in multiple sclerosis:
implications for exercise. Autonomic neuroscience: basic & clinical, 188, 82–85.
https://doi.org/10.1016/j.autneu.2014.10.017
Iorio, K. (2019).
Do fans make any difference in a heatwave? ABC News.
https://www.abc.net.au/news/2019-12-20/are-fans-completely-useless-in-a-
heatwave3f/11808944
Jeschke, M. G., Gauglitz, G. G., Kulp, G. A., Finnerty, C. C., Wil iams, F. N., Kraft, R., Suman,
O. E., Mlcak, R. P., & Herndon, D. N. (2011). Long-term persistance of the
pathophysiologic response to severe burn injury.
PloS one,
6(7), e21245.
https://doi.org/10.1371/journal.pone.0021245
Jost W. H. (2017). Autonomic Dysfunction in Parkinson's Disease: Cardiovascular Symptoms,
Thermoregulation, and Urogenital Symptoms.
International review of neurobiology, 134,
771–785. https://doi.org/10.1016/bs.irn.2017.04.003
Kim, S. H., Kim, J. S., Jin, M. H., & Lee, J. H. (2017). The effects of weather on pediatric
seizure: a single-center retrospective study (2005–2015).
Science of the total
environment, 609, 535-540.
King, K. (2023).
Ducted Air Conditioning vs Split System. Canstar Blue.
https://www.canstarblue.com.au/appliances/ducted-vs-split-system-air-con-the-pros-
and-cons/
Laique, M. B., & Hussain, T. (2018). Comparison Between Traditional Air Conditioning System
and Wearable Cooling/Heating Devices.
International Journal of Engineering Research
and Technology,
7(1), 111-113.
Landero J. (2014). Postural orthostatic tachycardia syndrome: a dermatologic perspective and
successful treatment with losartan.
The Journal of clinical and aesthetic dermatology,
7(8), 41–47 https:/ www.ncbi.nlm.nih.gov/pmc/articles/PMC4142820
Lenzer, B., Rupprecht, M., Hoffmann, C., Hoffmann, P., & Liebers, U. (2020). Health effects of
heating, ventilation and air conditioning on hospital patients: a scoping review.
BMC
public health,
20(1), 1287. https://doi.org/10.1186/s12889-020-09358-1
Lockyer, K. (2023).
Portable Air Conditioner vs Split System. Canstar Blue.
https://www.canstarblue.com.au/appliances/portable-or-split-system-air-conditioning-
the-pros-and-cons/
Lohner, S. (2017).
Chil ing Science: Evaporative Cooling with Liquids. Scientific American.
https://www.scientificamerican.com/article/chilling-science-evaporative-cooling-with-
liquids/
Page 413 of 425
FOI 24/25- 0013
Milne, G., Reardon, C., Ryan, P., Pavia, M., & Wyndham, J. (2020).
Heating and cooling. Your
Home: Australian Government. https://www.yourhome.gov.au/energy/heating-and-
cooling
Morris, N. B., Chaseling, G. K., English, T., Gruss, F., Maideen, M. F. B., Capon, A., & Jay, O.
(2021). Electric fan use for cooling during hot weather: a biophysical modelling study.
The Lancet Planetary Health, 5(6), e368-e377. https:/ doi.org/10.1016/S2542-
5196(21)00136-4
Mullane, J. (2023).
How Much Does Ducted Air Conditioning Cost? Canstar Blue.
https://www.canstarblue.com.au/appliances/ducted-air-conditioning-cost
Nakayama, Y., Shimizu, T., Matsuda, C., Haraguchi, M., Hayashi, K., Mochizuki, Y., Nagao,
M., Kawata, A., & Isozaki, E. (2018). Non-motor manifestations in ALS patients with
tracheostomy and invasive ventilation.
Muscle & nerve,
57(5), 735–741.
https://doi.org/10.1002/mus.26004
Novello, B. J., & Pobre, T. (2023). Electrodiagnostic Evaluation of Peripheral Neuropathy. In
StatPearls. StatPearls Publishing.
Osil a, E. V., Marsidi, J. L., Shumway, K. R., & Sharma, S. (2023).
Physiology, Temperature
Regulation. In StatPearls. StatPearls Publishing.
https://www.ncbi.nlm.nih.gov/books/NBK507838/
Pfeiffer R. F. (2020). Autonomic Dysfunction in Parkinson's Disease. Neurotherapeutics : the
journal of the American Society for Experimental NeuroTherapeutics, 17(4), 1464–1479.
https://doi.org/10.1007/s13311-020-00897-4
Pollandt, S., & Bleck, T. P. (2018). Thermoregulation in epilepsy. Handbook of clinical
neurology, 157, 737–747. https://doi.org/10.1016/B978-0-444-64074-1.00045-8
Price, M. J., & Trbovich, M. (2018). Thermoregulation following spinal cord injury.
Handbook of
clinical neurology, 157, 799–820. https://doi.org/10.1016/B978-0-444-64074-1.00050-1
Raising Children Network. (2024). Sensory sensitivities & autism: 4-18 years.
https://raisingchildren.net.au/autism/behaviour/understanding-behaviour/sensory-
sensitivities-asd
Rakers, F., Walther, M., Schiffner, R., Rupprecht, S., Rasche, M., Kockler, M., ... & Schwab,
M. (2017). Weather as a risk factor for epileptic seizures: a case‐crossover study.
Epilepsia,
58(7), 1287-1295.
Razi, O., Tartibian, B., Teixeira, A. M., Zamani, N., Govindasamy, K., Suzuki, K., Laher, I., &
Zouhal, H. (2022). Thermal dysregulation in patients with multiple sclerosis during
SARS-CoV-2 infection. The potential therapeutic role of exercise.
Multiple sclerosis and
related disorders, 59, 103557. https://doi.org/10.1016/j.msard.2022.103557
Ren, S., Han, M., & Fang, J. (2022). Personal Cooling Garments: A Review.
Polymers,
14(24),
5522. https://doi.org/10.3390/polym14245522
Page 414 of 425
FOI 24/25- 0013
Richard, A., & Iredale, A. (2023).
What size air conditioner do you need? CHOICE
https://www.choice.com.au/home-and-living/cooling/air-conditioners/articles/what-size-
air-conditioner-do-i-need
Rodríguez-Sánchez, S., Valiente, N., Seseña, S., Cabrera-Pinto, M., Rodríguez, A., Aranda,
A., Palop, L., & Fernández-Martos, C. M. (2022). Ozone modified hypothalamic
signaling enhancing thermogenesis in the TDP-43A315T transgenic model of
Amyotrophic Lateral Sclerosis.
Scientific reports,
12(1), 20814.
https://doi.org/10.1038/s41598-022-25033-4
Romanovsky, A. A. (2018).
Thermoregulation Part I: From basic neuroscience to clinical
neurology. Elsevier.
Savvy. (2023). Air Conditioning Use in Australia. https://www.savvy.com.au/energy/air-
conditioning-use-in-australia
Shajahan, A., Culp, C. H., & Wil iamson, B. (2019). Effects of indoor environmental parameters
related to building heating, ventilation, and air conditioning systems on patients' medical
outcomes: A review of scientific research on hospital buildings.
Indoor air,
29(2), 161–
176. https://doi.org/10.1111/ina.12531
Stevens, C. J., Singh, G., Peterson, B., Vargas, N. T., & Périard, J. D. (2023). The effect of
cooling garments to improve physical function in people with multiple sclerosis: A
systematic review and meta-analysis.
Multiple sclerosis and related disorders, 78,
104912. https:/ doi.org/10.1016/j.msard.2023.104912
Strengers, Y., Dahlgren, K., Nichol s, L., Pink, S., Martin, R. (2021).
Digital Energy Futures:
Future Home Life. Emerging Technologies Research Lab (Monash University).
Melbourne, Australia.
https://www.monash.edu/ data/assets/pdf file/0011/2617157/DEF-Future-Home-Life-
Full-Report.pdf
Thompson, H. J., Tkacs, N. C., Saatman, K. E., Raghupathi, R., & McIntosh, T. K. (2003).
Hyperthermia following traumatic brain injury: a critical evaluation.
Neurobiology of
disease,
12(3), 163-173.
Thwaites, P. A., Gibson, P. R., & Burgell, R. E. (2022). Hypermobile Ehlers-Danlos syndrome
and disorders of the gastrointestinal tract: What the gastroenterologist needs to know.
Journal of gastroenterology and hepatology,
37(9), 1693–1709.
https://doi.org/10.1111/jgh.15927
Weydt, P., Dupuis, L., & Petersen, Å. (2018). Thermoregulatory disorders in Huntington
disease.
Handbook of clinical neurology, 157, 761–775. https://doi.org/10.1016/B978-0-
444-64074-1.00047-1
Wrigsley, K. (2023).
How much electricity does an air conditioner use? Canstar Blue.
https://www.canstarblue.com.au/appliances/how-much-electricity-does-aircon-use/
Page 415 of 425
FOI 24/25- 0013
Zander, K. K., Mathew, S., & Carter, S. (2024). Behavioural (mal) adaptation to extreme heat
in Australia: Implications for health and wellbeing.
Urban Climate, 53, 101772.
https://doi.org/10.1016/j.uclim.2023.101772
Zander, K. K., van Hoof, J., Carter, S., & Garnett, S. T. (2023). Living comfortably with heat in
Australia–preferred indoor temperatures and climate zones.
Sustainable Cities and
Society, 104706. https://doi.org/10.1016/j.scs.2023.104706
Zaniboni, L., & Toftum, J. (2023). Indoor environment perception of people with autism
spectrum condition: a scoping review.
Building and Environment, 110545.
Zawadzka, M., Szmuda, M., & Mazurkiewicz-Bełdzińska, M. (2017). Thermoregulation
disorders of central origin - how to diagnose and treat.
Anaesthesiology intensive
therapy,
49(3), 227–234. https:/ doi.org/10.5603/AIT.2017.0042
Zhang Y. (2019). Thermoregulation following Spinal Cord Injury: Theory and Fact.
Medicine
and science in sports and exercise,
51(11), 2425.
https://doi.org/10.1249/MSS.0000000000002086
Zhong, G., Bolitho, S., Grunstein, R., Naismith, S. L., & Lewis, S. J. (2013). The relationship
between thermoregulation and REM sleep behaviour disorder in Parkinson's disease.
PloS one,
8(8), e72661. https:/ doi.org/10.1371/journal.pone.0072661
Page 416 of 425