FOI 23/24 - 1008
Page 37 of 76
FOI 23/24 - 1008
Page 38 of 76

FOI 23/24 - 1008
Page 39 of 76
FOI 23/24 - 1008
Page 40 of 76
FOI 23/24 - 1008
Page 41 of 76
FOI 23/24 - 1008
Page 42 of 76
FOI 23/24 - 1008
Page 43 of 76
FOI 23/24 - 1008
Page 44 of 76

FOI 23/24 - 1008
Page 45 of 76

FOI 23/24 - 1008
Page 46 of 76
FOI 23/24 - 1008
Page 47 of 76

FOI 23/24 - 1008
Page 49 of 76
FOI 23/24 - 1008
Page 51 of 76
FOI 23/24 - 1008
Page 52 of 76
FOI 23/24 - 1008
Page 55 of 76
FOI 23/24 - 1008
Page 56 of 76
FOI 23/24 - 1008
Page 57 of 76

FOI 23/24 - 1008
Page 58 of 76
 DOCUMENT 4
DOCUMENT 4
FOI 23/24 - 1008
Research Request – Functional Seizures
Provide research on functional seizures, AKA non epileptic seizures,
psychogenic non-epileptic seizures (PNES) or pseudo seizures in the following
areas:
•
Brief
Assessment criteria that should be met to confirm the diagnosis.
• Functional implications of PNES e.g. How does it show up for an
individual.
• Treatment recommendations with specific evidence on Cognitive
Behavioural Therapy.
Date
August 02, 2019
Requester
Shannon S22(1)(a)(ii) - irr
Researcher
Craig S22(1)(a)(ii) -
Contents
Summary ................................................................................................................................................. 2
What are Psychogenic non-epileptic seizures (PNES) ............................................................................. 2
Functional Implications ........................................................................................................................... 3
Overview ............................................................................................................................................. 3
How the person may present during a PNES ...................................................................................... 3
Personality Disorders/Traits ............................................................................................................... 4
Diagnosis Criteria .................................................................................................................................... 5
Overview ............................................................................................................................................. 5
Clinical Judgement .............................................................................................................................. 5
Early signs of PNES .............................................................................................................................. 5
Treatment Recommendations ................................................................................................................ 6
Overview ............................................................................................................................................. 6
Cognitive Behavioural Therapy (CBT) ................................................................................................. 6
Reference List .......................................................................................................................................... 8
R e s e a r c h R e q u e s t - F u n c t i o n a l S e i z u r e s
P a g e |
1
Page 59 of 76

FOI 23/24 - 1008
Summary
• The most commonly used term for the condition is Psychogenic non-epileptic seizures
(PNES).
• There is extensive literature and research on the subject and many public/community
oriented support groups exist globally for those experiencing the condition.
• Whilst there appears to be much understanding and clarity with regard to the functional
impairments commonly associated with the condition, there is little clarity regarding
guidelines or practice for the diagnosis of the condition, with video electroencephalogram
(vEGG) appearing to be the gold standard diagnostic tool, but even this is questioned (This is
explained further below). However, the general signs/indicators of an individual potentially
having the condition appears to be clear.
• There are no clear guidelines or practice for the treatment of the condition. However, a
review of available literature clearly indicates that there is success in the use of Cognitive
Behavioural Therapy (CBT) as a treatment.
• Research in this area is continuing to date, and there is a general “excitement” amongst
health professionals and those with the condition, of CBT being a promising treatment.
What are Psychogenic non-epileptic seizures (PNES)
The Australian government funded service HealthDirect website which links to Epilepsy Action
Australia, identifies Psychogenic non-epileptic seizures (PNES) as one of the three major categories
of seizures.
Psychogenic non-epileptic seizures have been labelled many names. Some common terms used are:
• Pseudo seizures
• Dissociative seizures
• Non epileptic events
• Non epileptic attack disorder (NEAD)
• Functional neurological disorder (FND)
• Conversion disorder (psychiatric diagnosis)
PNES are a physical symptom of a psychological disturbance and are usually involuntary.
They are ‘sudden, involuntary changes in behaviour, sensation, motor activity, cognitive processing
(can include change in level of consciousness) or autonomic function (e.g. blood pressure, heart rate)
linked to psychological or social distress.’ These events look like epileptic seizures, but are not
caused by abnormal electrical discharges in the brain. They are often triggered by an emotional or
psychological cause rather than a physiological one and can be seen in people with or without
epilepsy. PNES function as a coping mechanism. Research indicates that people with these events
are more likely to use poor coping strategies to handle stress. 1
1 Epilepsy Action Australia, “Psychogenic non-epileptic seizures", [website], 2017 https://www.epilepsy.org.au/epilepsy-trainer-news-
feature-psychogenic-non-epileptic-seizures, (accessed August 01 2019).
R e s e a r c h R e q u e s t - F u n c t i o n a l S e i z u r e s P a g e |
2
Page 60 of 76

FOI 23/24 - 1008
Functional Implications
Overview
A person experiencing PNES may have changes in behaviour, sensation, motor activity, cognitive
processing, blood pressure and heart rate with psychological or social distresses 2. A narrative
systematic synthesis of qualitative research identified five themes reflecting the experiences of
those with the condition: seizure events, diagnosis, treatment and management, emotional events,
and the impact of PNES on daily life. The research found that people experiencing the condition
shared the following common traits associated with their wellbeing:
• Getting diagnosis and being misdiagnosed
• Getting quality treatment and management for the condition
• Extreme emotional events and difficulty in processing emotions
• Stress with general uncertainty surrounding the condition
• Negative experiences with healthcare professionals were common
• Significant burdens associated with financial losses
• Psychosocial losses
• Difficulties in not being "heard" by health care professionals
• Commonality of past traumas, such as sexual, emotional and physical abuse
• Other impacts on daily life (family, friends, reclusing, feelings of being a burden,
employment difficulties). 3
A Flinders University Australia cohort research study explored the psychosocial effects of PNES,
finding that individuals have feelings of confusion and isolation. PNES may be triggered by anxiety,
psychological tension and heightened defence against intense emotions. In some cases PNES may be
a result of psychological trauma, previous psychiatric history, physical and sexual abuse or
posttraumatic stress disorder. People diagnosed with PNES feel anger, shame, helplessness, and
experience suicidal ideation. 4
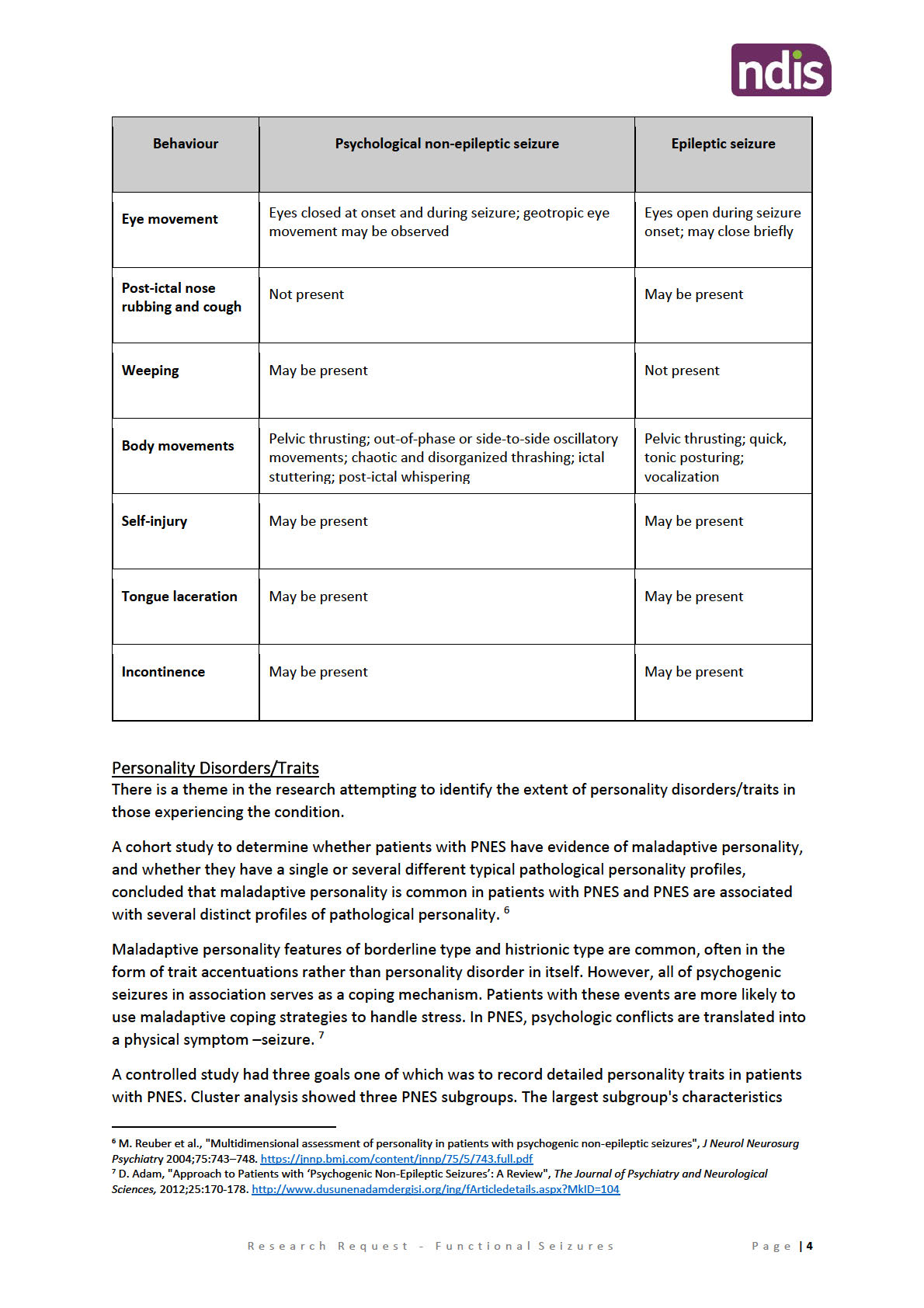
How the person may present during a PNES
In a research article by Curt LaFrance MD, Director of Neuropsychiatry at Rhode Island Hospital,
PNES can be difficult to distinguish from epileptic seizures (ES), with both showing alterations in
behaviour, consciousness, sensation, and perception5. The table below shows how a person may
present whilst experiencing a PNES episode:
2 Epilepsy Action Australia, “Psychogenic non-epileptic seizures", [website], 2017 https://www.epilepsy.org.au/epilepsy-trainer-news-
feature-psychogenic-non-epileptic-seizures, (accessed August 01 2019).
3 G. Rawlings and M. Reuber, “What patients say about living with psychogenic nonepileptic seizures: A systematic synthesis of qualitative
studies”, Academic Neurology Unit, University of Sheffield, UK, 2016. https://www.seizure-journal.com/article/S1059-1311(16)30116-
9/pdf
4 A.Thimm and M. Bellon, "The psychosocial effects of psychogenic non-epileptic seizures (PNES),
The epilepsy report, issue 2, 2011, pp. 5-6
http://www.epilepsyaustralia.net/uploads/74689/ufiles/PDF/issue-2-2011.pdf
5 W. LaFrance MD, Eye-opening behaviors help diagnose nonepileptic seizures, Current Psychiatry. 2006 November;5(11):121-130
https://mdedge-files-live.s3.us-east-2.amazonaws.com/files/s3fs-public/Document/September-2017/0511CP_Neuroscience.pdf
R e s e a r c h R e q u e s t - F u n c t i o n a l S e i z u r e s P a g e |
3
Page 61 of 76
FOI 23/24 - 1008
Page 62 of 76

FOI 23/24 - 1008
resembled borderline personality, with high scores on all dimensions. This subgroup had an 83.7%
chance of continued PNES at follow-up. The third-largest subgroup's characteristics resembled
avoidant personality disorder, with increases in all but the dissocial behaviour scores. 8
Diagnosis Criteria
Overview
No clinical guidelines for diagnosis could be found, and there is much in the research and literature
indicating the difficulty in the diagnosis and misdiagnosis of the condition. “The diagnosis of PNES
can be challenging and requires careful evaluation to exclude true epileptic seizures or other medical
conditions that cause seizures. Neither epileptic nor non epileptic seizures should be dealt with as a
diagnosis of exclusion—they may coexist. 9
Video EEG (vEGG)
Research on the diagnosis and assessment of PNES indicates that video EEG is the most significant
diagnostic tool. Prolonged video EEG monitoring is considered the gold standard for diagnosis, but
sometimes it can take a long time to get this organised. 10 However, there also appears to be a
theme of non-consensus within the research, where video EEG is also considered restrictive. “It can
be concluded that no EEG criterion is sufficient to make an unequivocal diagnosis of PNES. An
abnormal inter-ictal EEG may be considered as a positive indication of epilepsy but has no
significance for the diagnosis PNES.” 11
Clinical Judgement
There are many health professionals asserting that clinical judgement can be a sufficient method of
assessing PNES, where the importance of obtaining detailed history and physical examination of
patients presenting with epileptic seizures is paramount. By understanding the nature of PNES in
patients with disorders masquerading as epilepsy, more effective treatment can be given, even in
cases when the diagnosis of coexistent epileptic seizures has already been established. 12
There are also schools of thought amongst health professionals in the arena, that the practice of
relying only on vEEG is insufficient. While research shows that epileptiform discharges can elude the
vEEG, other studies reveal that the test is considered the gold standard by experts for differentiating
ES from PNES. It does not capture all epileptiform discharges, but the vEEG is still employed as a
litmus test. 13
Early signs of PNES
A GP may suspect PNES if:
• Antiepileptic medication does not reduce or stop the seizures
• The seizures are always triggered by an emotional or stress response
8 G. Fricchione, et al., "Personality Traits in Psychogenic Non-Epileptic Seizures vs. Epileptic Seizures",
J Neurol Neurosurg Psychiatry, May
2004. https://www.jwatch.org/jn200408060000004/2004/08/06/personality-traits-psychogenic-non-epileptic
9 Epilepsy Action Australia, “Psychogenic non-epileptic seizures", [website], 2017 https://www.epilepsy.org.au/epilepsy-trainer-news-
feature-psychogenic-non-epileptic-seizures, (accessed August 01 2019).
10 “Psychogenic non-epileptic seizures", [website], 2017 https://www.epilepsy.org.au/epilepsy-trainer-news-feature-psychogenic-non-
epileptic-seizures, (accessed August 01 2019).
11 J. Kuyk et al., "The diagnosis of psychogenic non-epileptic seizures: a review",
Seizure. 1997 August 6(4):243-53.
https://www.sciencedirect.com/science/article/pii/S1059131197800726
12 S. Ali, "How to Use Your Clinical Judgment to Screen for and Diagnose Psychogenic Nonepileptic Seizures without Video
Electroencephalogram
", Innov Clin Neurosci. 2011 Jan: 8(1): 36–42. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3036551
13 C. Carlson, "A Proposed Etiology of Psychogenic Nonepileptic Seizures
", J Neurol Psychiatr Disord 1(1): 201, 2019.
http://www.scienceinquest.com/open-access/pdf/jnpd/a-proposed-etiology-of-psychogenic-nonepileptic-seizures.pdf
R e s e a r c h R e q u e s t - F u n c t i o n a l S e i z u r e s P a g e |
5
Page 63 of 76

FOI 23/24 - 1008
• The seizures usually occur in the presence of others
• The characteristics of seizures are inconsistent with epileptic seizures. For
• example, side-to-side head shaking, eyelid fluttering, cycling movements of the legs, pelvic
thrusting, back arching, weeping, stuttering and talking and verbally responding
• There are usually no injuries or incontinence
• There is often a history of trauma, abuse or some form of psychiatric disorder such as
depression or post-traumatic stress disorder (PTSD) 14
Treatment Recommendations
Overview
No clinical guidelines for treatments could be found. Epilepsy Action Australia suggests treatment of
PNES should consist of psychological or psychiatric intervention and that there is now a recent shift
towards also using physical therapy in combination with psychotherapy. They also suggest that the
following need to be determined:
• Are there triggering or maintaining factors that are important, and to try to manage these.
For example, is there an ongoing physical trigger that can be treated (for example pain, a
neurological illness like migraine, etc.)?
• Is there depression that can be treated? Are there specific psychological issues that the
person feels are relevant and would like to explore?
• Is there some form of ongoing stress that needs to be managed?
• Some people find benefit from complementary treatments such as meditation, hypnosis and
acupuncture.
• About 60 to 70 percent of people find benefits from physical therapies and rehabilitation
based on an understanding of their condition.
Epilepsy Action Australia also advises that PNES can be supported by various principles of
neuropsychological interventions, including
Cognitive Behavioural Therapy for any comorbid
depression and anxiety, and various principles of neuro physiotherapy interventions, adding that
medication management should be very restricted and mainly used to relieve the symptoms of
comorbid anxiety or depression. 15
Cognitive Behavioural Therapy (CBT)
There is a rising trend in the literature indicating the use of and success of CBT in the treatment of
PNES.
A clinical trial in 2014 set out to evaluate different PNES treatments compared with standard
medical care (treatment as usual). The trial looked at the response of people who received the
following treatments: Sertraline, a commonly used antidepressant medication, a form of
cognitive
behavioural therapy, a form of
cognitive behavioural therapy and sertraline, and Standard medical
care. The trial showed that:
• CBT helped improve frequency of non-epileptic seizures in over half of the people who used
this treatment.
14 Epilepsy Action Australia, “Psychogenic non-epileptic seizures", [website], 2017 https://www.epilepsy.org.au/epilepsy-trainer-news-
feature-psychogenic-non-epileptic-seizures, (accessed August 01 2019).
15 Epilepsy Action Australia, “Psychogenic non-epileptic seizures", [website], 2017 https://www.epilepsy.org.au/epilepsy-trainer-news-
feature-psychogenic-non-epileptic-seizures, (accessed August 01 2019).
R e s e a r c h R e q u e s t - F u n c t i o n a l S e i z u r e s P a g e |
6
Page 64 of 76

FOI 23/24 - 1008
• People treated with a form of CBT alone had a significant improvement in seizures – their
seizure frequency decreased by 51.4% after treatment as compared to before treatment.
Secondary measures (depression, anxiety, functioning, and quality of life) also improved. 16
A case report this year (2019) presented a case of a 24 year old male with a severe PTSD condition.
When PTSD was suspected a diagnosis was confirmed via video-EEG. The patient underwent
supervised withdrawal of antiepileptic medications with the initiation of CBT, which reduced the
frequency of seizures. The report suggests that the diagnosis of PNES can present as a challenge and
failure to diagnose its psychological nature can lead to a delay in the psychological intervention. CBT
leads to a decrease in seizure frequency, and improvement in psychiatric symptoms, psychosocial
functioning, and quality of life. It is important to consider PNES in the differential diagnosis of
seizures presented by psychiatric patients, as CBT is necessary for better patient outcomes. 17
A much referenced randomized controlled trial in 2010 set out to compare CBT and standard
medical care as treatments for PNES, and concluded that compared with standard medical care,
cognitive-behavioural therapy significantly reduced seizure activity in patients with psychogenic non-
epileptic seizures. 18
16 W. LaFrance Jr, et el., "Multicenter Pilot Treatment Trial for Psychogenic Nonepileptic Seizures: A Randomized Clinical Trial
", JAMA
Psychiatry, 2014:71(9):997-1005. https://jamanetwork.com/journals/jamapsychiatry/fullarticle/1884286
17 S. Kamil et al., "Cognitive Behavioral Therapy (CBT) in Psychogenic Non-Epileptic Seizures (PNES): A Case Report and Literature Review",
Behav Sci (Basel). 2019 Jan 29;9(2). https://www.ncbi.nlm.nih.gov/pubmed/30699899
18 L. Goldstein et al., "Cognitive-behavioral therapy for psychogenic nonepileptic seizures: A pilot RCT",
Neurology, 2010 Jun 15; 74(24).
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2905892
R e s e a r c h R e q u e s t - F u n c t i o n a l S e i z u r e s P a g e |
7
Page 65 of 76

FOI 23/24 - 1008
Reference List
A.Thimm and M. Bellon, "The psychosocial effects of
Cohort Research
psychogenic non-epileptic seizures (PNES),
The epilepsy report, issue 2, 2011, pp. 5-6
Study Full Review
http://www.epilepsyaustralia.net/uploads/74689/ufiles/PDF/issue-2-2011.pdf
C. Carlson, "A Proposed Etiology of Psychogenic Nonepileptic Seizures
", J Neurol Psychiatr
Research Review
Disord 1(1): 201, 2019. http://www.scienceinquest.com/open-access/pdf/jnpd/a-proposed-
etiology-of-psychogenic-nonepileptic-seizures.pdf
D. Adam, "Approach to Patients with ‘Psychogenic Non-Epileptic Seizures’: A Review",
The
Research Review.
Journal of Psychiatry and Neurological Sciences, 2012;25:170-178.
http://www.dusunenadamdergisi.org/ing/fArticledetails.aspx?MkID=104
Epilepsy Action Australia, “Psychogenic non-epileptic seizures", [website], 2017
Website
https://www.epilepsy.org.au/epilepsy-trainer-news-feature-psychogenic-non-epileptic-seizures,
(accessed August 01 2019).
G. Fricchione, et al., "Personality Traits in Psychogenic Non-Epileptic Seizures vs. Epileptic
Research Review
Seizures
", J Neurol Neurosurg Psychiatry, May 2004.
https://www.jwatch.org/jn200408060000004/2004/08/06/personality-traits-psychogenic-non-
epileptic
G. Rawlings and M. Reuber, “What patients say about living with psychogenic nonepileptic
Narrative systematic
seizures: A systematic synthesis of qualitative studies”, Academic Neurology Unit, University of
synthesis of
Sheffield, UK, 2016. https://www.seizure-journal.com/article/S1059-1311(16)30116-9/pdf
qualitative research.
Full document
J. Kuyk et al., "The diagnosis of psychogenic non-epileptic seizures: a review",
Seizure. 1997
Research Review
August 6(4):243-53. https://www.sciencedirect.com/science/article/pii/S1059131197800726
L. Goldstein et al., "Cognitive-behavioral therapy for psychogenic nonepileptic seizures: A pilot
Randomized
RCT",
Neurology, 2010 Jun 15; 74(24).
Controlled Trial
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2905892
M. Reuber et al., "Multidimensional assessment of personality in patients with
Cohort Study. Full
psychogenic non-epileptic seizures",
J Neurol Neurosurg Psychiatry, 2004; 75:743–748.
paper.
https://jnnp.bmj.com/content/jnnp/75/5/743.full.pdf
S. Ali, "How to Use Your Clinical Judgment to Screen for and Diagnose Psychogenic Nonepileptic
Literature Review.
Seizures without Video Electroencephalogram", Innov Clin Neurosci. 2011 Jan: 8(1): 36–42.
Full article.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3036551
S. Kamil et al., "Cognitive Behavioral Therapy (CBT) in Psychogenic Non-Epileptic Seizures
Case Report and
(PNES): A Case Report and Literature Review", Behav Sci (Basel). 2019 Jan 29; 9(2).
Literature Review
https://www.ncbi.nlm.nih.gov/pubmed/30699899
W. LaFrance Jr, et el., "Multicenter Pilot Treatment Trial for Psychogenic Nonepileptic Seizures:
Clinical Trial. Pilot
A Randomized Clinical Trial
", JAMA Psychiatry, 2014:71(9):997-1005.
Study
https://jamanetwork.com/journals/jamapsychiatry/fullarticle/1884286
W. LaFrance MD, “Eye-opening behaviors help diagnose nonepileptic seizures”,
Full research review
Current Psychiatry. 2006 November;5(11):121-130
article
https://mdedge-files-live.s3.us-east-2.amazonaws.com/files/s3fs-public/Document/September-
2017/0511CP Neuroscience.pdf
R e s e a r c h R e q u e s t - F u n c t i o n a l S e i z u r e s P a g e |
8
Page 66 of 76
 DOCUMENT 5
DOCUMENT 5
FOI 23/24 - 1008
Research – Treatment of Advanced Osteoarthritis, Spinal Stenosis
and Functional Neurological Disorder
AAT Matter – Access
Applicant (54 year old woman) is seeking Access and has diagnoses of:
• Advanced Osteoarthritis (Left Hip)
Brief
• Spinal Stenosis
• Functional Neurological Disorder
What are the known available and appropriate evidence based clinical, medical
or other treatments/interventions for each impairment listed above?
Date
September 16, 2020
Requester
Naomi S22(1)(a)(ii)
- irrele (Sen
ior Technical Advisor – TAB/AAT)
Researcher
Craig S22(1)(a)(ii) - ir(Tact
ical Research Advisor – TAB/AAT)
Please note:
The research and literature reviews collated by our TAB Research Team are not to be shared external to the Branch. These
are for internal TAB use only and are intended to assist our advisors with their reasonable and necessary decision-making.
Delegates have access to a wide variety of comprehensive guidance material. If Delegates require further information on
access or planning matters they are to call the TAPS line for advice.
The Research Team are unable to ensure that the information listed below provides an accurate & up-to-date snapshot of
these matters.
Contents
Related TAB Research ............................................................................................................................. 2
Summary ................................................................................................................................................. 2
Definitions ............................................................................................................................................... 3
Advanced Osteoarthritis (Left Hip) ..................................................................................................... 3
Spinal Stenosis .................................................................................................................................... 3
Functional Neurological Disorder ....................................................................................................... 3
Treatment ............................................................................................................................................... 4
Advanced Osteoarthritis (Left Hip) ..................................................................................................... 4
Physical Activity/Exercise ................................................................................................................ 5
Weight Management ...................................................................................................................... 5
Medications .................................................................................................................................... 5
Spinal Stenosis .................................................................................................................................... 6
Research– Treatment of Advanced Osteoarthritis, Spinal Stenosis and Functional Neurological Disorder
Page 1 of 10
Page 67 of 76

FOI 23/24 - 1008
Medication ...................................................................................................................................... 6
Physiotherapy ................................................................................................................................. 6
Steroid Injections ............................................................................................................................ 6
Laminectomy Surgery ..................................................................................................................... 7
Functional Neurological Disorder (FND) ............................................................................................. 7
Neuro-psychiatry & Neuro-psychology ........................................................................................... 8
Physical therapy .............................................................................................................................. 8
Occupational therapy ...................................................................................................................... 8
Medications .................................................................................................................................... 8
References .............................................................................................................................................. 9
Related TAB Research
NED19/326570: RES HWB Functional Neurological Disorder & CRPS 2019/0060 ADO283
(Research to assist Assessors from NAWM with their decisions for access requests relating to these
specific conditions).
Summary
Research indicates that all three conditions are best treated by a multi-disciplinary approach.
Treatment for Advanced Osteoarthritis (Left Hip)
Multi-disciplinary approach is taken with treatment which includes physical activity, weight
management, medication, and nondrug pain relief techniques to control pain and complementary
and alternative therapies. Australian GPs generally demonstrate a conservative approach, where
non-pharmacological interventions were not given the importance suggested by clinical practice
guidelines.
Treatment for Spinal Stenosis
Multi-disciplinary approach to treatment which may include medication, physiotherapy, steroids
injections, and laminectomy surgery as a last resort (where clinical treatment fails or neurological
symptoms worsen).
Treatment for Functional Neurological Disorder
Comprehensive multi-disciplinary team approach involving neurology, neuro-psychiatry, physical
therapy, occupational therapy, and Neuro-psychology.
Research– Treatment of Advanced Osteoarthritis, Spinal Stenosis and Functional Neurological Disorder Page 2 of 10
Page 68 of 76

FOI 23/24 - 1008
Definitions
Advanced Osteoarthritis (Left Hip)
Osteoarthritis (AO) is the most common form of arthritis. It occurs when the protective cartilage that
cushions the ends of your bones wears down over time. Although osteoarthritis can damage any
joint, the disorder most commonly affects joints in hands, knees, hips and spine. [1] Advanced and
terminal stage hip OA causes severe restriction of hip range of motion and hip pain. [2]
Spinal Stenosis
Spinal stenosis, or spinal canal stenosis, is a narrowing of the canal in which the spinal cord sits. The
narrowing can put pressure on the nerves in the back, which can cause pain and weakness in the
arms or legs.
Spinal stenosis is usually caused by arthritis. Some people are born with a narrowed spinal canal,
which puts them at greater risk. Spinal stenosis can happen after a disc prolapse (a ‘slipped disc’, or
a problem with the spongy discs between the bones of the spine).
Spinal stenosis can also be caused when a thickened ligament bulges into the spinal cord, by a
tumour, or by an injury to the back.
The most common form of spinal stenosis is in the lower back (called a lumbar stenosis). It can also
happen at the top of the spine (called a cervical stenosis). [3]
Functional Neurological Disorder
Functional neurologic disorders is a newer and broader term that includes what some people call
conversion disorder. It feature nervous system (neurological) symptoms that can't be explained by a
neurological disease or other medical condition. However, the symptoms are real and cause
significant distress or problems functioning.
Signs and symptoms vary, depending on the type of functional neurologic disorder, and may include
specific patterns. Typically these disorders affect movement of the senses, such as the ability to
walk, swallow, see or hear. Symptoms can vary in severity and may come and go or be persistent.
However, the patient can't intentionally produce or control the symptoms.
The cause of functional neurologic disorders is unknown. The condition may be triggered by a
neurological disorder or by a reaction to stress or psychological or physical trauma, but that's not
always the case. Functional neurologic disorders are related to how the brain functions, rather than
damage to the brain's structure (such as from a stroke, multiple sclerosis, infection or injury). [4]
Research– Treatment of Advanced Osteoarthritis, Spinal Stenosis and Functional Neurological Disorder Page 3 of 10
Page 69 of 76

FOI 23/24 - 1008
Treatment
Advanced Osteoarthritis (Left Hip)
It appears a multi-disciplinary approach is taken with treatment. The Australian Institute of Health
and Welfare (AIHW) suggests that at present, there is no cure for osteoarthritis (OA) and the disease
is long-term and progressive. [5] The Institute suggests treatment for OA aims to manage symptoms,
increase mobility and maximise quality of life. General practitioners (GPs) are usually the first point
of contact with the health care system for people with OA and are ideally placed to play the role of
care coordinator to ensure treatment continuity. GP management of OA may include assessment
and diagnosis, referral to other health services, prescribing medication and providing education
about the condition.
Treatment options [5] for OA include:
• physical activity
• weight management
• medication
• joint replacement surgery
Other sources [6] also suggest the following inclusions in treatment plans:
• Rest and joint care
• Use of a Crutches, Canes, and Walkers to take weight off the affected hip
• Nondrug pain relief techniques to control pain
• Complementary and alternative therapies
It would appear that the severity of the OA would determine the likely treatment protocol. A 2016
study [7] looked at International evidence-based guidelines for the management of patients with hip
and knee OA which recommend to start with a combination of non-surgical treatments, and using
surgical intervention only if a patient does not respond sufficiently to non-surgical treatment
options. Despite the recommendations, there are strong indications that nonsurgical treatments are
not optimally used in orthopaedic practice.
In Australia, a 2015 survey study set out to examine opinions about the management of OA by
Australian GPs following the release of the Royal Australian College of General Practitioners
Guideline for the non-surgical management of hip and knee. The study concluded that Australian
GPs generally demonstrated a conservative approach to the treatment of OA, and non-
pharmacological interventions were not given the importance that is suggested by clinical practice
guidelines. [8]
The Royal Australian College of General Practitioners Guideline for the non-surgical management of
hip and knee best practice [9], for long term and advanced stage management are:
Long term management of OA
Best practice management of chronic conditions:
• optimal use of medicines
• non-pharmacological management
Research– Treatment of Advanced Osteoarthritis, Spinal Stenosis and Functional Neurological Disorder Page 4 of 10
Page 70 of 76

FOI 23/24 - 1008
• care and referral pathways
• patient self-management education
• patient psychosocial support requirements
Treatment and management in advanced stages of OA
Best practice management to optimise quality of life:
• optimal use of medicines
• non-pharmacological management
• care and referral pathways
• patient self-management education
• patient psychosocial support requirements
• Carer support and information
Physical Activity/Exercise
Exercise is an important and effective component in both management and prevention of OA.
Exercise helps improve symptoms (especially pain and joint stiffness) and quality of life by increasing
range of motion (the ability to move joints through their full motion), strengthening muscles around
affected joints, assists in weight control and reduces risk of other chronic diseases (e.g. diabetes and
cardiovascular disease). Exercise is also beneficial for other comorbidities and overall health. A GP or
Exercise Physiologist should be consulted before undertaking an exercise program. [5]
Weight Management
Being overweight increases the risk of developing OA, due to the increased load on weight bearing
joints and increased stress on cartilage. Weight management is strongly recommended for people
with knee and/or hip OA who are overweight or obese. For people with existing OA and who are
overweight or obese, weight loss can help reduce symptoms. Weight loss should be combined with
exercise for the greatest benefits. A GP or Dietitian can be consulted to discuss weight
loss/management strategies. [5]
Medications
Treatment of OA with medication aims to relieve pain, reduce inflammation and improve functioning
and quality of life. Analgesics, or pain medications, are commonly used to manage the pain of OA.
Analgesics include paracetamol, non-steroidal anti-inflammatory drugs (NSAIDs) and opioid
analgesics. For those with hip and/or knee OA requiring pain relief, it may be reasonable to trial the
use of paracetamol or NSAIDs for a short period and then discontinue use if it is not effective.
Corticosteroid injections may also be recommended for short term pain relief for hip and/or knee
OA if appropriate. Opioids are not recommended for the treatment of hip and/or knee OA. [5]
Research– Treatment of Advanced Osteoarthritis, Spinal Stenosis and Functional Neurological Disorder Page 5 of 10
Page 71 of 76

FOI 23/24 - 1008
Spinal Stenosis
Research indicates a multi-disciplinary approach to treatment which may include:
• Medication (for pain management)
• Physiotherapy (build strength, flexibility and balance)
• Steroids injections (reduce pain and inflammation)
• Laminectomy surgery (where other treatments don’t work) [10]
Medication
In a 2016 literature review [11], suggest that drug treatment does not offer many possibilities. The
indiscriminate and frequent use of anti-inflammatory medications for chronic lumbar pain does not
have a proven satisfactory response and may be associated with gastrointestinal and renal
complications. Its use should be very restricted and avoided in elderly patients with narrow lumbar
spinal canal syndrome.
Simple painkillers, muscle relaxants, and opioids may be of value. They are indicated for treating and
controlling the pain but have no effect on the treatment of neurogenic claudication. [11] Gabapentin
has been shown to be a safe medication; it may be taken orally and has a positive effect on patients
with neurogenic claudication and the sensory alterations, which are very common in this cohort of
patients [11]. Corticosteroids are also used indiscriminately. The idea is that there is an inflammatory
process associated with the mechanical compression that could benefit from the medication, but
this theory was not proven. [11]
Physiotherapy
Physiotherapy, or more broadly rehabilitation is a non-surgical approach. Manual therapy,
stretching, and muscular strengthening play an important role, in addition to the exercises. Patients
who suffer from canal stenosis have, in addition to pain, a significant muscle loss, which severely
limits their activities and progressively worsens their clinical condition, which leads to further
impairments. [12] [13]
The recommended activities include manual therapy, strengthening, and walking training, as well as
exercises that improves proprioception. In addition, weight loss is important, because obese patients
have been described to have a worse prognosis. [14]. Cycling is a very much recommended activity,
not only because patients tolerate it well, but it also allows them to improve their conditioning and
does not impact other joints that may also be degenerated, such as the hip and the knee. [15]
Steroid Injections
Peridural corticosteroids (Steroid injections) are another type of non-surgical treatment for narrow
lumbar spinal canal syndrome, as opposed to oral corticosteroids, which were shown to be
ineffective for this condition. [14]
Research– Treatment of Advanced Osteoarthritis, Spinal Stenosis and Functional Neurological Disorder Page 6 of 10
Page 72 of 76

FOI 23/24 - 1008
Peridural corticosteroids have some advantages. There are several possibilities for their
administration, with or without radioscopy, as well as several techniques: interlaminar, caudal, and
transforaminal. Despite their limited benefits, their use may have lasting efficacy in many patients.
[15]
Laminectomy Surgery
Surgical treatment is considered the last resort for patients with treating lumbar canal stenosis.
Because surgery is performed in patients over 65 years of age, there is significant morbidity and
mortality, which increase with associated diseases and patient age, making it mandatory to assess
the risks and benefit of the surgery.
Surgical treatment is indicated when clinical treatment fails or neurological symptoms worsen. There
are several different surgical techniques.
• The classical technique is laminectomy, performed by an incision along the midline followed
by decompression, removing up to 50% of facets.
• Interspinous spacers have been recently included in the surgical arsenal for canal stenosis,
but studies are still under way, and there are no studies yet evaluating for an adequate
follow-up period.
For this reason, the actual benefit of this kind of surgery is not yet well established. However, it is
known that it does offer some advantages, such as short hospitalization periods and limited
bleeding. [16]
Functional Neurological Disorder (FND)
Research indicates that FND is best treated within a comprehensive multi-disciplinary team involving
[17] [18]:
• Neurology
• Neuro-psychiatry
• Physical therapy
• Occupational therapy and,
• Neuro-psychology
• Speech pathology
• Physiotherapists
Patients with physical symptoms (gait disturbance, weakness, paralysis, dystonia, etc.) will often
need physical treatment. Allied health professionals including: speech pathologist, occupational
therapists and physiotherapists then becomes integral to the patient’s recovery process. [18]
Patients who have early access to an FND specialised multi-disciplinary treatment program with
specialist FND knowledge, have the best chance of improved outcomes and potential for recovery.
When patients were able to access specialised treatment there were noticeable positive benefits.
[19]
Research– Treatment of Advanced Osteoarthritis, Spinal Stenosis and Functional Neurological Disorder Page 7 of 10
Page 73 of 76

FOI 23/24 - 1008
Neuro-psychiatry & Neuro-psychology
Around one third of patients with FND have a comorbid psychiatric condition [18]. Some patients
experience depression and anxiety as a result of having their functional symptoms. For others, a
history of trauma or adverse childhood experiences can make them vulnerable to developing FND.
Psychologists and psychiatrists can assist in the management of comorbid mental health conditions
and in the treatment of FND. Cognitive behavioural therapy (CBT) is an evidenced based
psychological approach for treating FND. This can include exploring the symptoms and identifying
behaviours and cognitions (thoughts) that maintain or exacerbate the symptoms to increase the
patient’s awareness of their symptoms. A range of CBT strategies can be taught to the patient to
assist them manage their FND and mood symptoms to maximise their everyday function. [18]
Physical therapy
Neuro-physiotherapists can offer education, movement retraining and self-management strategies.
Recent research has demonstrated marked improvements in functional motor symptoms in patients
who work closely with physiotherapists. [18]
Occupational therapy
Occupational therapists are able to build good rapport with patients and help them with self
explorations to understand what they can/can’t do, as well as, determining and addressing the
specific blockages for their normal everyday functioning. This is done through a wide range of
activities and relaxation techniques. [18]
Medications
Generally, pharmacological therapy for FND is avoided when possible. In the clinical practice, their
use may not be welcomed by many patients due to psychiatric stigma, perception of addictive and
harmful properties, and side effects. Antidepressants have demonstrated benefits even in those who
do not have comorbid mental disorders. Tricyclics are helpful in those with insomnia and pain.
Serotonin reuptake inhibitors are good for hypersomnia but not so good in pain management.
Neuropathic analgesia such as gabapentin or pregabalin are used in chronic pain. Patients are often
explained to that they can get better without the tablets but they are worth trying for those who are
looking to explore every therapeutic avenue. [18]
Research– Treatment of Advanced Osteoarthritis, Spinal Stenosis and Functional Neurological Disorder Page 8 of 10
Page 74 of 76

FOI 23/24 - 1008
References
1
Mayo Clinic. Osteoarthritis - Symptoms and causes [Internet]. 2020 [cited 15
September 2020]. Available from: https://www.mayoclinic.org/diseases-
conditions/osteoarthritis/symptoms-causes/syc-20351925
2
Teramoto Y, Fukushima K, Koyama T, Ohashi Y, Uchiyama K, Takahira N et al. Impact
of Jiggling Exercise as Conservative Treatment for Hip Osteoarthritis: A Report of Two
Cases. Case Reports in Orthopedics. 2020;2020:1-5.
3
Healthdirect.gov.au. Spinal stenosis [Internet]. 2020 [cited 15 September 2020].
Available from: https://www.healthdirect.gov.au/spinal-stenosis
4
Mayo Clinic. Functional neurologic disorders/conversion disorder - Symptoms and
causes [Internet]. 2020 [cited 15 September 2020]. Available from:
https://www.mayoclinic.org/diseases-conditions/conversion-disorder/symptoms-
causes/syc-20355197
5
Osteoarthritis, Treatment & management - Australian Institute of Health and Welfare
[Internet]. Australian Institute of Health and Welfare. 2020 [cited 15 September
2020]. Available from: https://www.aihw.gov.au/reports/chronic-musculoskeletal-
conditions/osteoarthritis/contents/treatment-management
6
WebMD. Hip Osteoarthritis (Degenerative Arthritis of the Hip) [Internet]. 2020 [cited
15 September 2020]. Available from: https://www.webmd.com/osteoarthritis/hip-
osteoarthritis-degenerative-arthritis-hip
7
Hofstede S, Marang-van de Mheen P, Vliet Vlieland T, van den Ende C, Nelissen R, van
Bodegom-Vos L. Barriers and Facilitators Associated with Non-Surgical Treatment Use
for Osteoarthritis Patients in Orthopaedic Practice. PLOS ONE. 2016;11(1):e0147406.
8
Basedow M, Williams H, Shanahan E, Runciman W, Esterman A. Australian GP
management of osteoarthritis following the release of the RACGP guideline for the
non-surgical management of hip and knee osteoarthritis. BMC Research Notes.
2015;8(1).
9
Royal Australian College of General Practitioners, Guideline for the non-surgical
management of hip and knee osteoarthritis [Internet]. Racgp.org.au. 2009 [cited 15
September 2020]. shorturl.at/efrR2
10
Healthdirect.gov.au. Spinal stenosis [Internet]. 2020 [cited 16 September 2020].
Available from: https://www.healthdirect.gov.au/spinal-stenosis
11
Rodrigues L. Lumbar Spinal Stenosis, Clinical Presentation, Diagnosis, and Treatment.
2016. DOI: 10.5772/63920
12
Rittemberg JD, Ross AE. Functional rehabilitation for degenerative lumbar spina
stenosis. Phys Med Rehabil Clin N Am (14);111–120, 2003.
13
Whtiman JM. Flyn TW, Frotz JM. Nonsurgical management of patients with lumbar
Research– Treatment of Advanced Osteoarthritis, Spinal Stenosis and Functional Neurological Disorder Page 9 of 10
Page 75 of 76

FOI 23/24 - 1008
spine stenosis: a literature review and a case series of three patients managed with
physical therapy. Phys Med Rehabil Clin N Am;14(1):77–101, 2003.
14
Rodrigues LC, Natour J. A double-blind, randomized controlled, prospective trial
assessing the effectiveness of oral corticoids in the treatment of symptomatic lumbar
canal stenosis. J Negat Results Bioemed;13:13, 2014.
15
Whitman JM, Flym TW, Chids JD, Wainer RS et al. A comparassion between two
physical therapy treatment programs for patients with lumbar spinal stenosis: a
randomized clinical trial. Spine;31(2):2541–2549, 2006.
16
Zucherman JF, Hsu KY, Hartjen CA, et al. A prospective randomized multicenter study
for the treatment of lumbar spinal stenosis with the X stop interspinous implant: 1-
year results. Eur Spine J;13:22–31, 2004.
17
FND Treatment Australia. FND Australia Support Services [Internet]. Fndaus.org.au.
2020 [cited 16 September 2020]. Available from: https://fndaus.org.au/fnd-
treatment-australia/
18
Mater Centre for Neuro Sciences. Functional Neurological Disorder (FND) Learning
guide [Internet]. Fndaustralia.com.au. 2020 [cited 16 September 2020]. Available
from: https://fndaustralia.com.au/resources/FND-Learning-guide-for-nurses.pdf
19
Mentalhealthcommission.gov.au. Consumer and Carer Experiences of fnd/Cd in
Australia [Internet]. 2019 [cited 16 September 2020]. Available from:
https://www.mentalhealthcommission.gov.au/getmedia/8ac49bb8-556e-42dc-b946-
a175149fb57d/Consumer-and-Carer-Experiences-of-FND-CD-in-Australia-FND-
Support-Services-Inc
Research– Treatment of Advanced Osteoarthritis, Spinal Stenosis and Functional Neurological Disorder
Page 10 of
10
Page 76 of 76