FOI 23/24 - 1008
Page 1 of 76
 DOCUMENT 2
[Resea
DOCUMENT 2
[Resea
FOI
rch paper
23/24 - 1008
]
OFFICIAL
For Internal Use Only
Functional neurological seizure disorder
The content of this document is OFFICIAL.
Please note:
The research and literature reviews collated by our TAB Research Team are not to be shared
external to the Branch. These are for internal TAB use only and are intended to assist our
advisors with their reasonable and necessary decision-making.
Delegates have access to a wide variety of comprehensive guidance material. If Delegates
require further information on access or planning matters, they are to call the TAPS line for
advice.
The Research Team are unable to ensure that the information listed below provides an
accurate & up-to-date snapshot of these matters
Research question: Provide research on functional seizures, AKA non epileptic seizures:
assessment criteria that should be met to confirm the diagnosis; functional implications of
PNES e.g. How does it show up for an individual?; treatment recommendations with specific
evidence on Cognitive Behavioural Therapy.
Date: 21/9/2022
Requestor: n/a review of previous TAB research
Endorsed by (EL1 or above):
Researcher: StephanieS22(1)(a)(ii)
- irrelevant mater
Cleared by: Stephanie S22(1)(a)(ii)
- irrelevant mat
1.
Contents
Functional neurological seizure disorder .................................................................................... 1
1.
Contents ....................................................................................................................... 1
2.
Summary ...................................................................................................................... 2
3.
Functional Neurological Seizure Disorder ..................................................................... 2
4.
Diagnosis ...................................................................................................................... 4
4.1
DSM-V clinical criteria ................................................................................................ 4
4.2
vEEG ......................................................................................................................... 5
4.3
Clinical assessment ................................................................................................... 6
5.
Presentation .................................................................................................................. 6
5.1
Functional Implications .............................................................................................. 6
Page 1 of 12
OFFICIAL
Page 2 of 76
 [Resea
[Resea
FOI
rch paper
23/24 - 1008
]
OFFICIAL
For Internal Use Only
5.2
Risk and prognostic factors ....................................................................................... 7
5.3
Presentation of functional neurological seizures vs epileptic seizures ....................... 7
6.
Treatment ..................................................................................................................... 8
6.1
Cognitive behaviour therapy ...................................................................................... 8
6.2
Psychoeducation ....................................................................................................... 9
6.3
Allied health therapy .................................................................................................. 9
6.4
Neuromodulation ..................................................................................................... 10
6.5
Medication ............................................................................................................... 10
7.
References ................................................................................................................. 11
2. Summary
This research is a review of the ‘Functional Seizures’ research paper completed by TAB
Tactical Research Team in 2019.
Functional neurological seizure disorder is listed under somatic symptom disorders in the
Diagnostic and Statistical Manual of Mental Disorders, 5th Ed. While it has previously been
considered a diagnosis of exclusion, advances in understanding of the disorder have enabled
the development of diagnostic criteria to confirm the diagnosis. Importantly, functional
neurological seizure disorder can co-occur with other neurological conditions such as epilepsy
and multiple sclerosis.
Functional neurological seizure disorder predominantly affects women. Functional symptoms
may result in motor deficits, sensory dysfunction and/or cognitive impairment. The prognosis
for functional neurological seizure disorder largely depends on the time to diagnosis and
adherence to the treatment plan. Cognitive behaviour therapy, psychoeducation, and allied
health support may have a role in the treatment of the disorder.
3. Functional Neurological Seizure Disorder
Functional neurological seizure disorder (FND) is one of the most common causes of
neurological disability (Medina et al, 2021). Functional neurological seizure disorder can
present and feel similar to epileptic seizures, but they are a physical symptom to a
psychological disturbance without any physiological connection to epilepsy and therefore sit
alongside somatic symptom disorders in the
Diagnostic and Statistical Manual of Mental
Page 2 of 12
OFFICIAL
Page 3 of 76
 [Resea
[Resea
FOI
rch paper
23/24 - 1008
]
OFFICIAL
For Internal Use Only
Disorders, 5th Ed. (DSM V) (American Psychiatric Association (APA), 2013; Epilepsy Action
Australia, 2020; Marcolini & Tolchin, 2021).
Historically, there have been multiple names for functional neurological seizure disorder in the
literature, including (Epilepsy Action Australia, 2020):
• Psychogenic non-epileptic seizure (PNES)
• Pseudo seizures
• Dissociative seizures
• Non epileptic events
• Non epileptic attack disorder (NEAD)
• Functional seizures
• Conversion disorder (psychiatric diagnosis)
The terms ‘functional neurological seizure disorder’ and ‘functional seizure’ are becoming more
commonly used as they are considered more neutral than some of the earlier terms that had
negative connotations for patients (Asadi-Pooya & Bazrafshan, 2020; Marcolini & Tolchin,
2021).
The true prevalence of functional neurological seizure disorder is not clear, however around
15% of presentations to general neurology clinics are attributed to functional neurological
seizure disorder (Ahmad & Ahmad, 2016; Forejtova et al, 2022; Maggio et al, 2020). Patients
are most commonly female, with initial presentation in their late teens to mid-twenties (Ahmad
& Ahmad, 2016; Kerr et al, 2021; Marcolini & Tolchin, 2021), although motor symptoms tend to
have their mean onset at ages 30-39 years (APA, 2013). Diagnosis prior to puberty is
uncommon, with approximately only 1% of patients who undergo video-
electroencephalography (vEEG) being diagnosed with the condition (Kerr et al, 2021).
People who experience functional neurological seizure disorder often have a history of trauma
or psychological stressors such as physical or sexual abuse, neglect, and social or family
conflict (Ahmad & Ahmad, 2016; APA, 2013; Marcolini & Tolchin, 2021). The condition is
associated with comorbid psychiatric and psychological difficulties, poor quality of life, elevated
mortality rates, and frequent use of the health system (Marcolini & Tolchin, 2021). Of note,
there has been found to be a strong relationship between fibromyalgia and functional
neurological seizure disorder, with one study in particular determining that out of 36 patients
diagnosed chronic pain or fibromyalgia, 27 were also found to have functional neurological
seizure disorder (Benbadis, 2005).
The prognosis for functional neurological seizure disorder can be poor, particularly when
treatment begins more than 6-12 months after symptom onset (Gill, 2019; Gupta & Lang, 2009).
Functional neurological seizure disorder can result in substantial physical disability (APA,
2013). The severity of long-term disability can be similar to that evident in people with other
Page 3 of 12
OFFICIAL
Page 4 of 76
 [Resea
[Resea
FOI
rch paper
23/24 - 1008
]
OFFICIAL
For Internal Use Only
significant neurological conditions such as multiple sclerosis, stroke and Parkinson’s disease
(APA, 2013; FND Australia, 2019).
4. Diagnosis
Functional neurological seizure disorder is often misdiagnosed for several years (Medina et al,
2021), the average delay being 7 to 10 years (Kerr et al, 2021; Marcolini & Tolchin, 2021).
Possibly due to the stigma of being a psychological condition, and a fear that doctors believe
the symptoms are due to malingering or fictitious disorder, patients often do not adhere to
treatment after diagnosis and remain high users of healthcare (Marcolini & Tolchin, 2021;
Medina et al, 2021).
Diagnosis of functional neurological seizure disorders should be based on a combination of
data, including: patient history and witness observations, clinical observations, and ictal (during
a neurological episode) and interictal (between episodes) electroencephalography (Asadi-
Pooya & Bazrafshan, 2020).
4.1 DSM-V clinical criteria
Functional neurological seizure disorder is classified as a conversion disorder in the chapter
‘Somatic Symptom and Related Disorders’ in the Diagnostic and Statistical Manual of Mental
Disorders 5th Edition (DSM-5). This set of diagnostic criteria emphasises the importance of
making a rule-in positive diagnosis rather than an exclusionary diagnosis that was common in
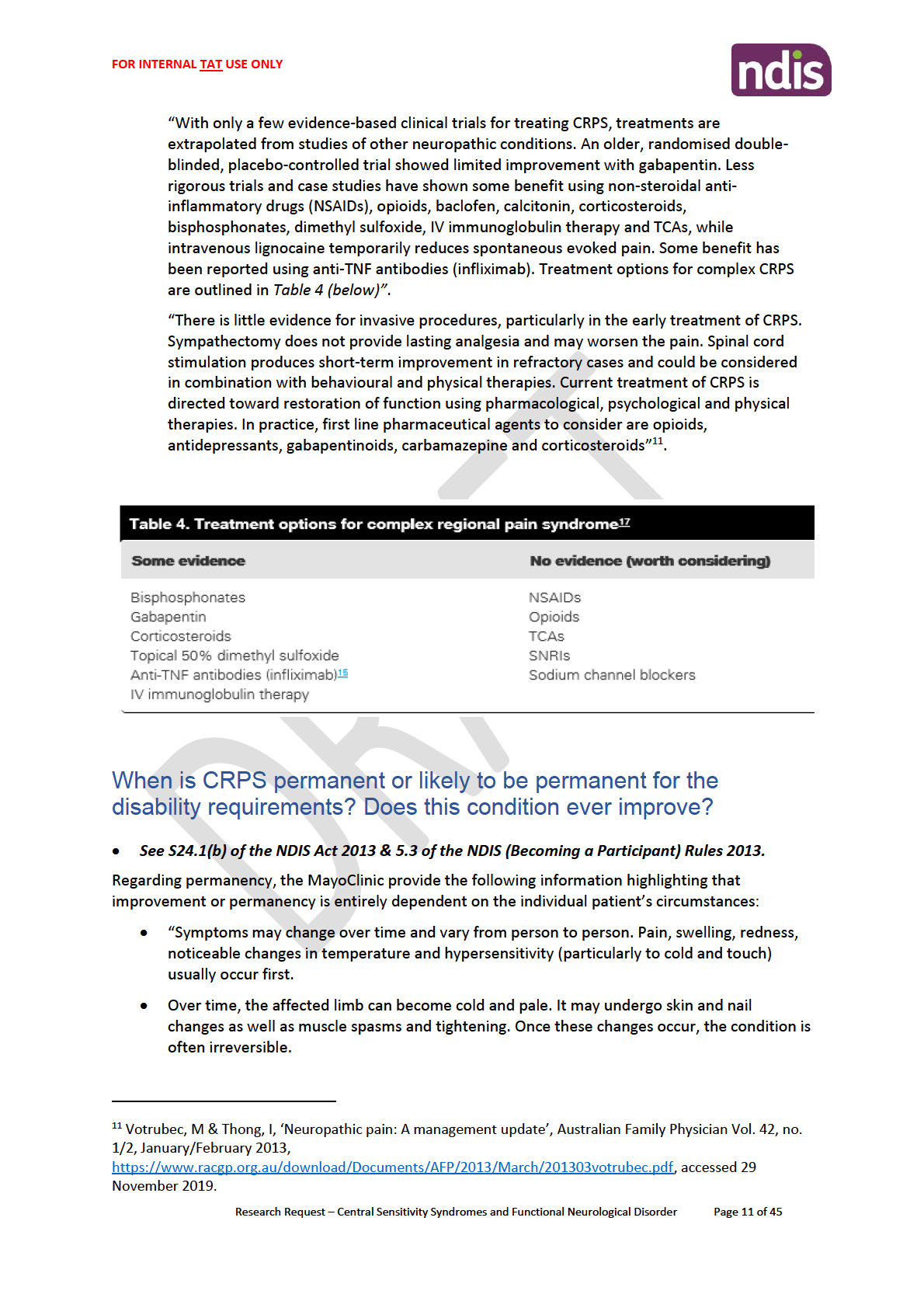
the past (Aybek & Perez, 2022). Table 1 outlines the diagnostic criteria for functional
neurological seizure disorder.
Table 1
DSM V diagnostic criteria for functional neurological disorder
DSM V Diagnostic criteria:
A. One or more symptoms of altered voluntary motor or sensory function
B. Clinical findings provide evidence of incompatibility between the symptom and
recognised neurological or medical conditions.
C. The symptom or deficit is not better explained by another medical or mental disorder.
D. The symptom or deficit causes clinically significant distress or impairment in social,
occupational, or other important areas of functioning and warrants medical evaluation.
The ICD-10-CM code depends on the symptom type:
Specify symptom type:
(F44.4) With weakness or paralysis
Page 4 of 12
OFFICIAL
Page 5 of 76
 [Resea
[Resea
FOI
rch paper
23/24 - 1008
]
OFFICIAL
For Internal Use Only
(F44.4) With abnormal movement (e.g., tremor, dystonia, myoclonus, gait disorder)
(F44.4) With swallowing symptoms
(F44.4) With speech symptom (e.g., dysphonia, slurred speech)
(F44.5) With attacks or seizures
(F44.6) With anaesthesia or sensory loss
(F44.6) With special sensory symptom (e.g., visual, olfactory, or hearing disturbance)
(F44.7) With mixed symptoms
Specify if:
Acute episode: Symptoms present for less than 6 months.
Persistent: Symptoms occurring for 6 months or more.
Specify if:
With psychological stressor
(specify stressor)
Without psychological stressor
Diagnosis of functional neurological seizure disorder relies on clinical evidence that shows the
symptoms of concern have not developed due to another recognised neurological disorder,
such as epilepsy. Importantly, an individual can be diagnosed with both functional neurological
seizure disorder and another neurological disease such as epilepsy or multiple sclerosis (APA,
2013).
Associated features that can support the diagnosis of functional neurological seizure disorder,
although not specific to the disorder, include (APA, 2013):
• a history of other functional somatic symptoms or disorders, particularly including pain
and fatigue
• onset that is associated with stress or trauma, either psychological or physical. Although
this temporal relationship may only be true for up to 50% of individuals
• ‘la belle indifference’ (i.e., the lack of concern about the implications of the symptom)
has been associated with functional neurological seizure disorder, but is not specific
and should not be used to make the diagnosis
4.2 vEEG
Video electroencephalography (vEEG) is the gold standard method to diagnose functional
neurological seizure disorder (Lopez & LaFrance, 2022; Marcolini & Tolchin, 2021). Extended
vEEG evaluations enable greater diagnostic certainty to capture seizure events without
epileptiform abnormalities immediately before, during or following seizures (Marcolini &
Tolchin, 2021). Compared to epileptic seizure waveforms, functional neurological seizure
Page 5 of 12
OFFICIAL
Page 6 of 76
 [Resea
[Resea
FOI
rch paper
23/24 - 1008
]
OFFICIAL
For Internal Use Only
disorder typically demonstrates normal awake brain electrical activity during impaired or lost
consciousness events (Marcolini & Tolchin, 2021). Extended vEEG can be performed in an
epilepsy monitoring unit; for individuals whose episodes are infrequent, single channel
electromyography can be obtained at home over weeks or months to support the diagnosis
(Marcolini & Tolchin, 2021).
4.3 Clinical assessment
An accurate diagnosis is best achieved using a combination of the patient history, information
from observers, physical examination, evaluation of ictal semiology with a normal ictal vEEG,
and psychiatric evaluation (Lopez & LaFrance, 2022; Marcolini & Tolchin, 2021).
There is no reliable laboratory test that is sensitive or specific to the diagnosis of functional
neurological seizure disorder (Marcolini & Tolchin, 2021). Currently, research suggests there
may be subtle differences in the structural and functional MRI of an individual with functional
neurological seizure disorder compared to a healthy control, however these results are
preliminary and cannot be used in clinical diagnosis or exclusion of functional neurological
seizure disorder (Marcolini & Tolchin, 2021).
5. Presentation
5.1 Functional Implications
Patients may present with motor and/or sensory or cognitive neurological symptoms (Barnett
et al, 2020) that can present acutely and resolve quickly or be long lasting (Nicholson et al,
2020). This results in a wide range of possible functional impairment, including (APA, 2013;
Barnett et al, 2020; Gill, 2019; Nhan & Cheah, 2020; Nicholson et al, 2020):
• Limb weakness or paralysis
• Gait disorders
• Balance problems
• Movement disorders such as tremor, jerks and dystonia
• Episodes of apparent unresponsiveness with or without limb movements, possibly
resembling epileptic seizures, syncope or coma
• Dysphagia
• Communication difficulties
• Speech disturbance, including reduced or absent speech volume, altered speech
articulation, prosody or fluency
• Fatigue
• Chronic pain
Page 6 of 12
OFFICIAL
Page 7 of 76
 [Resea
[Resea
FOI
rch paper
23/24 - 1008
]
OFFICIAL
For Internal Use Only
• Sensory symptoms such visual disturbances (e.g., double vision), cognitive symptoms
(e.g., planning difficulties, mental slowness, black outs, memory difficulties), tactile
disturbances (e.g., altered, reduced or absent skin sensation), or hearing disturbances
• Bladder and bowel problems
5.2 Risk and prognostic factors
The following are risk and prognostic factors associated with functional neurological seizures
(APA, 2013):
• Maladaptive personality traits, especially emotional instability, are common
• There may be a history of abuse and neglect
• Stressful life events, including physical injury, are common but not universal
• Other neurological diseases that cause similar symptoms, e.g., around 20% of
individuals with functional neurological symptom disorder also have epilepsy
• Individuals with functional neurological seizure disorder may show higher rates of
suicidal thoughts and attempts than individuals with a recognised neurological disease
• Short duration of symptoms and agreement with the diagnosis are positive prognostic
factors, whereas maladaptive personality traits, comorbid physical disease and receipt
of disability benefits appear to be negative prognostic factors
5.3 Presentation of functional neurological seizures vs epileptic seizures
People with functional neurological seizure disorder experience transient episodes of altered
awareness (Marcolini & Tolchin, 2021). The seizures are believed to be an involuntary coping
mechanism, and people who experience these types of seizure are more likely to use
maladaptive coping mechanisms to handle stress (Epilepsy Action Australia, 2020).
Differentiating functional neurological seizures from epileptic seizures can be difficult as both
show alterations in behaviour, consciousness, sensation and perception (Nhan & Cheah,
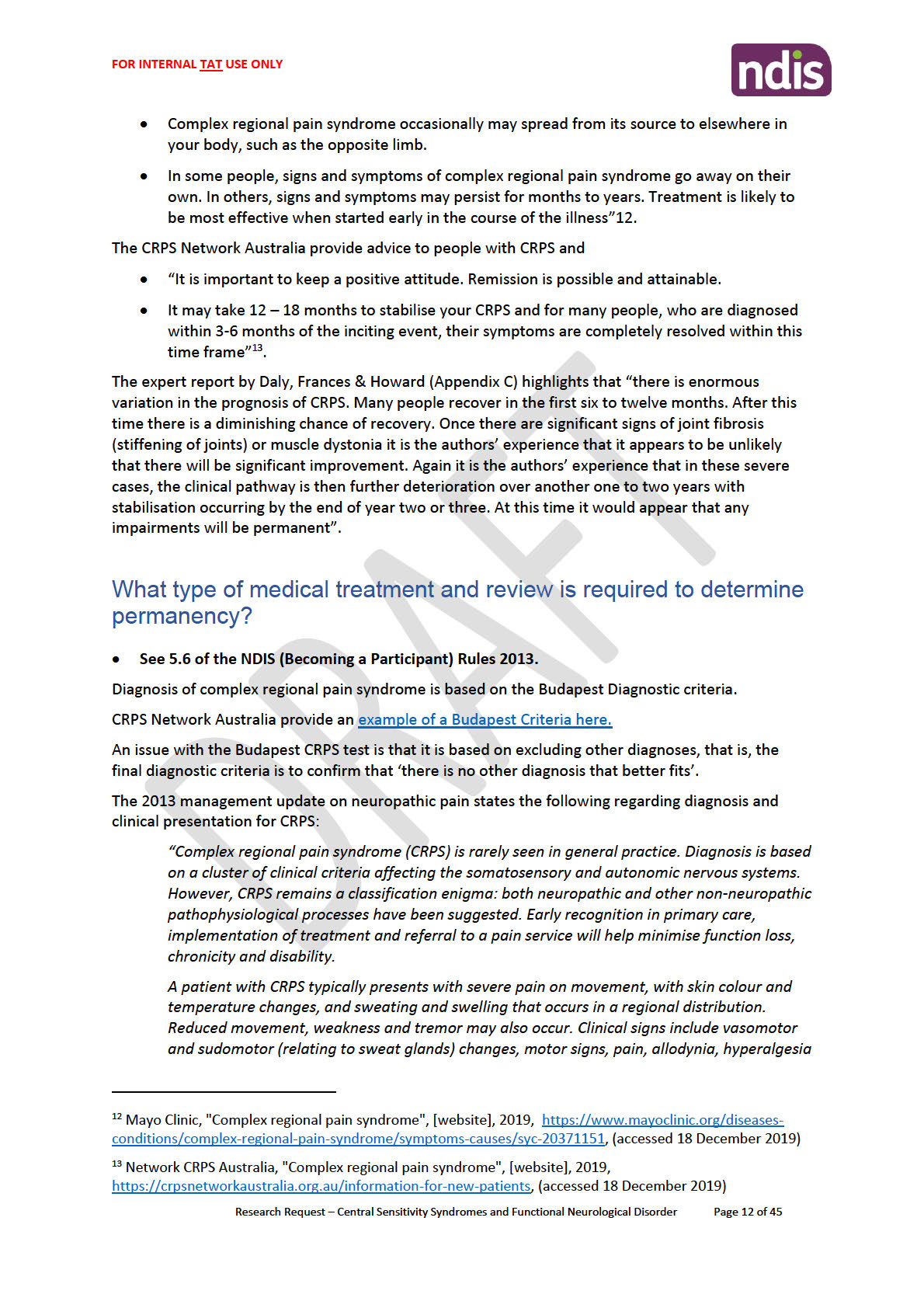
2020; Thimm & Belon, 2011). The table below highlights how a person may present during a
functional neurological seizure compared to an epileptic seizure (Nhan & Cheah, 2020; Thimm
& Belon, 2011):
Table 2
Functional neurological seizures versus epileptic seizures
Behaviour
Functional neurological seizure
Epileptic seizure
Page 7 of 12
OFFICIAL
Page 8 of 76
 [Resea
[Resea
FOI
rch paper
23/24 - 1008
]
OFFICIAL
For Internal Use Only
Duration over 5 mins
common
rare
Gradual onset
common
rare
Eyes and mouth closed
common
rare
Resisting eye opening
common
very rare
Post ictal weeping/upset
occasional
rare
Post ictal nose rubbing/cough
rare
occasional
Side to side head movements
common
rare
Type of body movements
Pelvic thrusting; out-of-phase or
Pelvic thrusting; quick,
side-to-side oscillatory movements;
tonic posturing;
chaotic and disorganized thrashing;
vocalization
ictal stuttering; post-ictal whispering
Respiration
often fast
ceases
Grunting sound
occasional
common
Recall for period of
common
very rare
unresponsiveness
Aura
common
common
Attacks rising from sleep
occasional
common
Self-injury
occasional
occasional
Tongue laceration
occasional
occasional
Incontinence
common
common
6. Treatment
In addition to treatment options, how the diagnosis is delivered and received influences
adherence to the treatment plan and therefore prognosis (Aybek et al, 2022; Marcolini &
Tolchin, 2021).
6.1 Cognitive behaviour therapy
Page 8 of 12
OFFICIAL
Page 9 of 76
 [Resea
[Resea
FOI
rch paper
23/24 - 1008
]
OFFICIAL
For Internal Use Only
A number of randomised controlled trials support the efficacy of cognitive behaviour therapy to
reduce seizure activity, improve psychosocial functioning, fewer somatic symptoms and
improve quality of life (Aybek et al, 2022; Marcolini & Tolchin, 2021), however long-term follow-
up generally indicated the effect did not remain significant (Aybek et al, 2022). A systematic
review of 11 studies investigating the efficacy of cognitive behaviour therapy for functional
neurological seizure disorder suggested moderate to large significant effects on measures of
physical symptoms, and small to moderate effect sizes for mental health, function and quality
of life (Gutkin et al, 2021). It was noted in this systematic review that the success of cognitive
behaviour therapy depends on the patient accepting their symptoms may relate to
psychological factors. Although Goldstein et al (2021) reported improvement in quality of life
and psychosocial functioning at 12 months, this was not 12 months post-cessation of therapy
but rather after the 12th month of therapy. Therefore, as reported by Aybek et al (2022), the
effect of the therapy may decrease over time which might suggest that individuals need to
have ongoing cognitive behaviour therapy for ongoing remission or decrease in symptoms.
6.2 Psychoeducation
While psychoeducation may not reduce seizure frequency, there is some evidence that it
improves psychosocial functioning as they develop greater understanding of their diagnosis,
acceptance and belief in the treatment plan (Aybek et al, 2022). An important consideration is
this effect may not be evident for online education and self-help interventions (Aybek et al,
2022). Implementing psychoeducation to improve understanding of the diagnosis may
encourage adherence to the treatment plan and increase the likelihood of better outcomes
(Medina et al, 2021).
6.3 Allied health therapy
Physiotherapy is the first treatment option for patients with motor symptoms, with an emphasis
on motor retraining (Aybek et al, 2022). Data from randomised controlled trials and
observational studies have demonstrated efficacy of physiotherapy for functional neurological
seizure disorder with improvements in gait, social functioning and quality of life reported
(Aybek et al, 2022; Maggio et al, 2020). Maggio et al (2020) reports an average of 34%
improvement in motor function was observed after adherence to weekly physiotherapy for an
average of 7 weeks.
Support from a speech therapist may be necessary for individuals who demonstrate speech,
language and swallowing impairments, however the efficacy and long-term outcomes after
speech and language therapy for individuals with significant impairment does not appear well
studied (Barnett et al, 2019).
A professional education paper by Nicholson et al (2020) has offered recommendations for the
role of occupational therapy for patients with functional neurological disorder. Occupational
therapy can provide practical support to overcome the effects of disability on activities of daily
living. This may include education, vocational rehabilitation, assistive technology assessment,
Page 9 of 12
OFFICIAL
Page 10 of 76
 [Resea
[Resea
FOI
rch paper
23/24 - 1008
]
OFFICIAL
For Internal Use Only
and strategies to overcome functional motor, visual and cognitive impairment (Nicholson et al,
2020).
6.4 Neuromodulation
Research into the efficacy of neuromodulation for functional neurological seizure disorder is
limited but emerging, therefore included in this research paper. As part of a systematic review,
Oriuwa et al (2022) analysed data from one paper investigation the effects of TMS on
functional seizures. All participants (N = 7) received high frequency repetitive stimulation of the
right temporoparietal junction for 30 sessions over 30 weeks, and all experienced a significant
decrease in weekly seizure frequency. At 3 months follow up, 4 participants had sustained
remission in seizure activity.
6.5 Medication
Antiseizure medications have no role in the treatment of functional neurological seizure
disorder, and may actually increase morbidity due to side effects (Lopez & LaFrance, 2022).
While individuals with functional neurological seizure disorder may be prescribed medication
for other psychological disorders, such as antidepressants, there is currently no medication to
prescribe specifically for the symptoms of functional neurological seizure disorder.
Page 10 of 12
OFFICIAL
Page 11 of 76
 [Resea
[Resea
FOI
rch paper
23/24 - 1008
]
OFFICIAL
For Internal Use Only
7. References
Aybek, S., & Perez, D. L. (2022). Diagnosis and management of functional neurological
disorder.
BMJ (Clinical research ed.),
376, o64. https://doi.org/10.1136/bmj.o64
Ahmad, O., & Ahmad, K. E. (2016). Functional neurological disorders in outpatient practice: An
Australian cohort.
Journal of clinical neuroscience : official journal of the Neurosurgical
Society of Australasia,
28, 93–96. https://doi.org/10.1016/j.jocn.2015.11.020
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental
disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
Asadi-Pooya, A. A., & Bazrafshan, M. (2020). Is patient acceptance of the diagnosis of
functional (psychogenic nonepileptic) seizures linked to their clinical
characteristics?.
Journal of psychosomatic research,
136, 110193.
https://doi.org/10.1016/j.jpsychores.2020.110193
Barnett, C., Armes, J., & Smith, C. (2019). Speech, language and swallowing impairments in
functional neurological disorder: a scoping review.
International journal of language &
communication disorders,
54(3), 309–320. https://doi.org/10.1111/1460-6984.12448
Barnett, C., Davis, R., Mitchell, C., & Tyson, S. (2020). The vicious cycle of functional
neurological disorders: a synthesis of healthcare professionals’ views on working with
patients with functional neurological disorder.
Disability and Rehabilitation.
DOI:10.1080/09638288.2020.1822935
Benbadis S. R. (2005). A spell in the epilepsy clinic and a history of "chronic pain" or
"fibromyalgia" independently predict a diagnosis of psychogenic seizures.
Epilepsy &
behavior,
6(2), 264–265. https://doi.org/10.1016/j.yebeh.2004.12.007
Epilepsy Action Australia. (2020).
Epilepsy trainer news: feature – psychogenic non-epileptic
seizures. Accessed from https://www.epilepsy.org.au/epilepsy-trainer-news-feature-
psychogenic-non-epileptic-seizures/
Forejtová, Z., Serranová, T., Sieger, T., Slovák, M., Nováková, L., Věchetová, G., Růžička, E.,
& Edwards, M. J. (2022). The complex syndrome of functional neurological
disorder.
Psychological medicine, 1–11. Advance online publication.
https://doi.org/10.1017/S0033291721005225
FND Australia. (2019).
Discover options for FND treatment in Australia. Accessed from
https://fndaus.org.au/fnd-treatment-australia/
Gill, K. (2019).
Consumer and carer experiences of FND/CD in Australia: The silent crisis.
Commissioned by the National Mental Health Commission, Sydney.
Goldstein, L. H., Robinson, E. J., Pilecka, I., Perdue, I., Mosweu, I., Read, H., et al. (2021).
Cognitive behaviour therapy compared with standardised medical care for adults with
dissociative non-epileptic seizures: the CODES RCT.
Health Technol Assess, 25(43).
Page 11 of 12
OFFICIAL
Page 12 of 76
 [Resea
[Resea
FOI
rch paper
23/24 - 1008
]
OFFICIAL
For Internal Use Only
Gupta, A., & Lang, A. E. (2009). Psychogenic movement disorders. Current Opinion in
Neurology, 22(4), 430-436. doi:10.1097/WCO.0b013e32832dc169
Kerr, W. T., Sreenivasan, S. S., Allas, C. H., Janio, E. A., Karimi, A. H., Dubey, I., D'Ambrosio,
S. R., Smith, J. M., Engel, J., Jr, Feusner, J. D., & Stern, J. M. (2021). Title: Functional
seizures across the adult lifespan: female sex, delay to diagnosis and
disability.
Seizure,
91, 476–483.
Lopez, M. R., & LaFrance, W. C. (2022). Treatment of Psychogenic Nonepileptic
Seizures.
Current neurology and neuroscience reports,
22(8), 467–474.
https://doi.org/10.1007/s11910-022-01209-3
Maggio, J. B., Ospina, J. P., Callahan, J., Hunt, A. L, Stephen, C. D., & Perez, D. L. (2020).
Outpatient physical therapy for functional neurological disorder: A preliminary feasibility
and naturalistic outcome study in a U.S. cohort.
J Neuropsychiatry Clin Neurosci,
32,
85–89. doi:10.1176/appi.neuropsych.19030068
Marcolini, E., & Tolchin, B. (2021). Functional seizures.
Emergency Medicine Clinics of North
America, 39(1), 123-132. https://doi.org/10.1016/j.emc.2020.09.007
Medina, M., Giambarberi, L., Lazarow, S. S., Lockman, J., Faridi, N., Hooshmad, F., Karasov,
A., & Bajestan, S. N. (2021). Using patient centred clinical neuroscience to deliver the
diagnosis of functional neurological disorder (FND): Results from an innovative
educational workshop.
Academic Psychiatry, 45, 185-189.
https://doi.org/10.1007/s40596-020-01324-8
Nhan, P., & Cheah, V. (2020).
Functional neurological disorder (FND) learning guide. Mater
Centre for Neurosciences. Accessed from https://fndaustralia.com.au/resources/FND-
Learning-guide-for-nurses.pdf
Nicholson, C., Edwards, M. J., Carson, A. J., Gardiner, P., Golder, D., Hayward, K.,
Humblestone, S., Jinadu, H., Lumsden, C., MacLean, J., Main, L., Macgregor, L.,
Nielsen, G., Oakley, L., Price, J., Ranford, J., Ranu, J., Sum, E., & Stone, J. (2020).
Occupational therapy consensus recommendations for functional neurological disorder.
J Neurol Neurosurg Psychiatry, 91, 1037-1045. doi:10.1136/jnnp-2019-322281
Oriuwa, C., Mollica, A., Feinstein, A., Giacobbe, P., Lipsman, N., Perez, D. L., & Burke, M. J.
(2022). Neuromodulation for the treatment of functional neurological disorder and
somatic symptom disorder: a systematic review.
Journal of neurology, neurosurgery,
and psychiatry,
93(3), 280–290. https://doi.org/10.1136/jnnp-2021-327025
Thimm, A., & Bellon, M. (2011). The psychosocial effects of psychogenic non-epileptic
seizures (PNES).
The Epilepsy Report, (2), 4-6.
Page 12 of 12
OFFICIAL
Page 13 of 76
FOI 23/24 - 1008
Page 14 of 76
FOI 23/24 - 1008
Page 15 of 76
FOI 23/24 - 1008
Page 16 of 76
FOI 23/24 - 1008
Page 17 of 76

FOI 23/24 - 1008
Page 18 of 76
FOI 23/24 - 1008
Page 19 of 76
FOI 23/24 - 1008
Page 20 of 76
FOI 23/24 - 1008
Page 21 of 76
FOI 23/24 - 1008
Page 22 of 76
FOI 23/24 - 1008
Page 23 of 76
FOI 23/24 - 1008
Page 24 of 76
FOI 23/24 - 1008
Page 25 of 76
FOI 23/24 - 1008
Page 26 of 76
FOI 23/24 - 1008
Page 27 of 76
FOI 23/24 - 1008
Page 28 of 76
FOI 23/24 - 1008
Page 29 of 76
FOI 23/24 - 1008
Page 30 of 76
FOI 23/24 - 1008
Page 31 of 76

FOI 23/24 - 1008
Page 32 of 76
FOI 23/24 - 1008
Page 33 of 76

FOI 23/24 - 1008
Page 34 of 76
FOI 23/24 - 1008
Page 35 of 76
FOI 23/24 - 1008
Page 36 of 76